Department of Epidemiology and International Public Health, Bielefeld School of Public Health, Bielefeld, Germany.
Department of General Practice and Health Services Research, University Hospital Heidelberg, Heidelberg, Germany.
BMJ Open. 2019 May 30;9(5):e027357. doi: 10.1136/bmjopen-2018-027357.
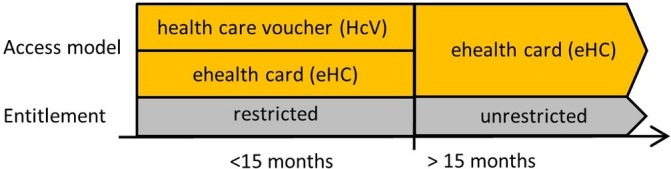
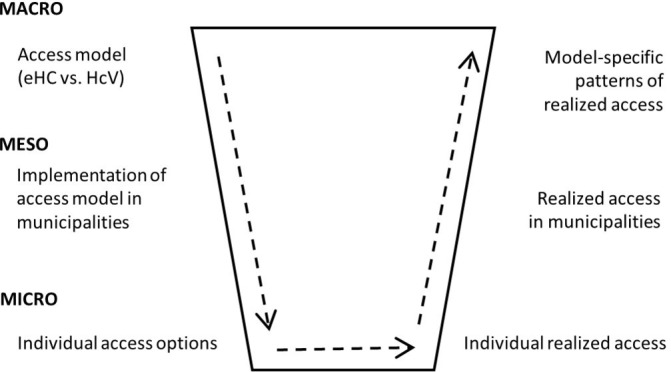
In many countries, including Germany, newly arriving refugees face specific entitlement restrictions and access barriers to healthcare. While entitlement restrictions apply to all refugees who seek protection in Germany during the first months, the barriers to access depend on the model that the states and the municipalities implement locally. Currently, two different models exist: the healthcare voucher model (HcV) and the electronic health card model (eHC). The aim of the study is to analyse the consequences of these two different access models on newly arrived refugees' realised access to healthcare.
The random assignment of refugees to municipalities allows for a quasi-experimental design by comparing realised access to healthcare among refugees in six municipalities in North Rhine-Westphalia which have implemented HcV or eHC. We compare realised access to healthcare using ambulatory care sensitive conditions and health expenditure as outcome indicators, and use of emergency care, preventive care, psychotherapeutic or psychiatric care, and of therapeutic devices as process indicators. Results will be adjusted for aggregated information on age, sex, socioeconomic structure of the municipalities and density of general practitioners or specialists.
We cooperated with local welfare offices and the statutory health insurance for data collection. Thereby, we were able to avoid recruiting large numbers of refugee patients immediately after arrival while their access and entitlement to healthcare are restricted. We developed an extensive data protection concept and ensured that all data collected are fully anonymised. Results will be published in peer-reviewed journals and summarised in reports to the funding agency.
在许多国家,包括德国,新抵达的难民在获得医疗保健方面面临特定的权利限制和准入障碍。虽然权利限制适用于在头几个月内在德国寻求保护的所有难民,但准入障碍取决于各州和市政府在当地实施的模式。目前,存在两种不同的模式:医疗券模式(HcV)和电子健康卡模式(eHC)。本研究的目的是分析这两种不同的准入模式对新抵达难民实际获得医疗保健的影响。
难民被随机分配到各市镇,这使得通过比较北莱茵-威斯特法伦州六个实施 HcV 或 eHC 的市镇中难民的实际医疗保健获得情况,可以进行准实验设计。我们使用门诊治疗敏感条件和卫生支出作为结果指标,使用急诊、预防保健、心理治疗或精神病治疗以及治疗设备作为过程指标来比较实际获得的医疗保健情况。结果将根据各市镇的年龄、性别、社会经济结构以及普通医生或专家的密度的汇总信息进行调整。
我们与当地福利办公室和法定健康保险公司合作进行数据收集。通过这种方式,我们能够避免在难民入境后立即招募大量患者,因为他们的医疗保健准入和权利受到限制。我们制定了广泛的数据保护概念,并确保收集的所有数据都完全匿名。研究结果将发表在同行评议的期刊上,并总结报告给资助机构。