Physical Performance Service Line, G 3/5/7, US Army Office of the Surgeon General, Falls Church, VA, USA.
Baylor University, Road, Bldg 2841, Suite 1301; JBSA Fort Sam Houston, Stanley, TX, 3630, USA.
BMC Musculoskelet Disord. 2019 Jun 1;20(1):266. doi: 10.1186/s12891-019-2646-5.
One of the reported goals of hip preservation surgery is to prevent or delay the onset of osteoarthritis. This includes arthroscopic surgery to manage Femoroacetabular Impingement (FAI) Syndrome. The purpose of this study was to describe the prevalence of clinically-diagnosed hip OA within 2 years after hip arthroscopy for FAI syndrome, and 2) determine which variables predict a clinical diagnosis of OA after arthroscopy.
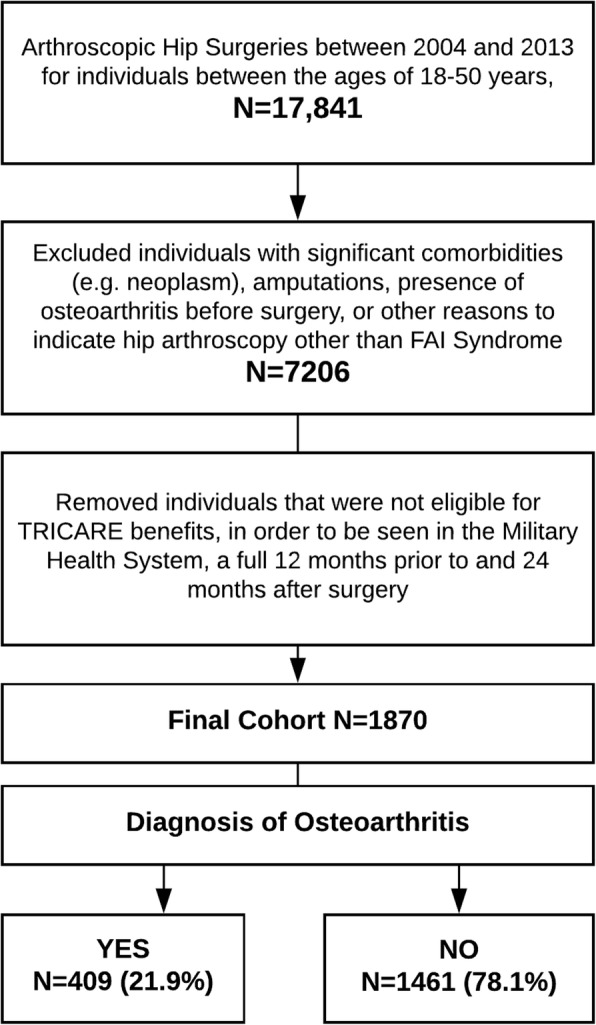
Observational analysis of patients undergoing hip arthroscopy between 2004 and 2013, utilizing the Military Health System Data Repository. Individuals with prior cases of osteoarthritis were excluded. Presence of osteoarthritis was based on diagnostic codes rendered by a medical provider in patient medical records. Adjusted odds ratios (95% CI) for an osteoarthritis diagnosis were reported for relevant clinical and demographic variables.
Of 1870 participants in this young cohort (mean age 32.2 years), 21.9% (N = 409) had a postoperative clinical diagnosis of hip osteoarthritis within 2 years. The 3 significant predictors in the final model were older age (OR = 1.04; 95%CI = 1.02, 1.05), male sex (OR = 1.31; 95%CI = 1.04, 1.65), and having undergone an additional hip surgery (OR = 2.33; 95% CI = 1.72, 3.16). Military status and post-surgical complications were not risk factors.
A clinical diagnosis of hip osteoarthritis was found in approximately 22% of young patients undergoing hip arthroscopy in as little as 2 years. These rates may differ when using alternate criteria to define OA, such as radiographs, and likely underestimate the prevalence. A more comprehensive approach, considering various criteria to detect OA will likely be necessary to accurately identify the true rates. Females were at lower risk, while increasing age and multiple surgeries increased the risk for an OA diagnosis. OA onset still occurs after "hip preservation" surgery in a substantial number of individuals within 2 years. This should be considered when estimating rates of disease prevention after surgery. Prospective trials with sound methodology are needed to determine accurate rates and robust predictors of osteoarthritis onset after hip preservation surgery.
髋关节保存手术的一个目标是预防或延迟骨关节炎的发生。这包括关节镜手术来治疗股骨髋臼撞击综合征(FAI)。本研究的目的是描述髋关节镜治疗 FAI 综合征后 2 年内临床诊断为骨关节炎的发生率,以及 2)确定哪些变量可以预测关节镜检查后的 OA 临床诊断。
利用军事卫生系统数据存储库对 2004 年至 2013 年间接受髋关节镜手术的患者进行观察性分析。排除有骨关节炎既往病史的患者。根据病历中医疗服务提供者的诊断代码确定是否存在骨关节炎。报告了与相关临床和人口统计学变量相关的骨关节炎诊断的调整优势比(95%CI)。
在这个年轻队列的 1870 名参与者中(平均年龄 32.2 岁),21.9%(N=409)在术后 2 年内临床诊断为髋关节骨关节炎。最终模型中的 3 个显著预测因素是年龄较大(OR=1.04;95%CI=1.02,1.05)、男性(OR=1.31;95%CI=1.04,1.65)和接受了额外的髋关节手术(OR=2.33;95%CI=1.72,3.16)。军事地位和术后并发症不是危险因素。
在接受髋关节镜手术的年轻患者中,大约 22%在 2 年内被诊断为髋关节骨关节炎。当使用替代标准(如 X 光片)来定义 OA 时,这些比率可能会有所不同,并且可能会低估发病率。为了准确识别真实的发病率,可能需要采用更全面的方法,考虑各种标准来检测 OA。女性的风险较低,而年龄增加和多次手术会增加 OA 诊断的风险。在 2 年内,大量接受“髋关节保存”手术后的个体仍会出现 OA 发作。在估计手术后疾病预防的发生率时应考虑到这一点。需要进行具有良好方法学的前瞻性试验,以确定髋关节保存手术后 OA 发作的准确发生率和稳健预测因素。