Trommer Maike, Yeo Sin Yuin, Persigehl Thorsten, Bunck Anne, Grüll Holger, Schlaak Max, Theurich Sebastian, von Bergwelt-Baildon Michael, Morgenthaler Janis, Herter Jan M, Celik Eren, Marnitz Simone, Baues Christian
Faculty of Medicine and University Hospital Cologne, Department of Radiation Oncology and Cyberknife Center, University of Cologne, Cologne, Germany.
Faculty of Medicine and University Hospital Cologne, Radio Immune-Oncology Consortium, University of Cologne, Cologne, Germany.
Front Pharmacol. 2019 May 14;10:511. doi: 10.3389/fphar.2019.00511. eCollection 2019.
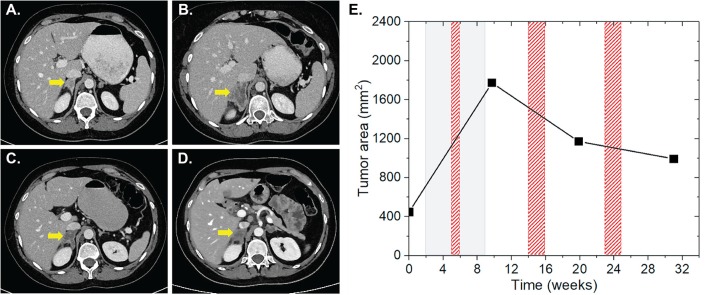
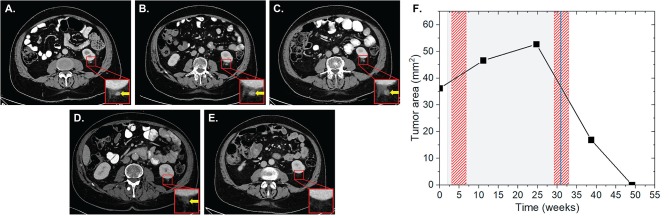
Immune checkpoint inhibition (ICI) targeting the programmed death receptor 1 (PD-1) has shown promising results in the fight against cancer. Systemic anti-tumor reactions due to radiation therapy (RT) can lead to regression of non-irradiated lesions (NiLs), termed "abscopal effect" (AbE). Combination of both treatments can enhance this effect. The aim of this study was to evaluate AbEs during anti-PD-1 therapy and irradiation. We screened 168 patients receiving pembrolizumab or nivolumab at our center. Inclusion criteria were start of RT within 1 month after the first or last application of pembrolizumab (2 mg/kg every 3 weeks) or nivolumab (3 mg/kg every 2 weeks) and at least one metastasis outside the irradiation field. We estimated the total dose during ICI for each patient using the linear quadratic (LQ) model expressed as 2 Gy equivalent dose (EQD2) using α/β of 10 Gy. Radiological images were required showing progression or no change in NiLs before and regression after completion of RT(s). Images must have been acquired at least 4 weeks after the onset of ICI or RT. The surface areas of the longest diameters of the short- and long-axes of NiLs were measured. One hundred twenty-six out of 168 (75%) patients received ICI and RT. Fifty-three percent (67/126) were treated simultaneously, and 24 of these (36%) were eligible for lesion analysis. AbE was observed in 29% (7/24). One to six lesions (mean = 3 ± 2) in each AbE patient were analyzed. Patients were diagnosed with malignant melanoma (MM) ( = 3), non-small cell lung cancer (NSCLC) ( = 3), and renal cell carcinoma (RCC) ( = 1). They were irradiated once ( = 1), twice ( = 2), or three times ( = 4) with an average total EQD2 of 120.0 ± 37.7 Gy. Eighty-two percent of RTs of AbE patients were applied with high single doses. MM patients received pembrolizumab, NSCLC, and RCC patients received nivolumab for an average duration of 45 ± 35 weeks. We demonstrate that 29% of the analyzed patients showed AbE. Strict inclusion criteria were applied to distinguish the effects of AbE from the systemic effect of ICI. Our data suggest the clinical existence of systemic effects of irradiation under ICI and could contribute to the development of a broader range of cancer treatments.
靶向程序性死亡受体1(PD-1)的免疫检查点抑制(ICI)在抗癌斗争中已显示出有前景的结果。放射治疗(RT)引起的全身抗肿瘤反应可导致未受照射病灶(NiLs)消退,称为“远隔效应”(AbE)。两种治疗方法联合使用可增强这种效应。本研究的目的是评估抗PD-1治疗和放射治疗期间的远隔效应。我们筛选了在我们中心接受派姆单抗或纳武单抗治疗的168例患者。纳入标准为在首次或最后一次应用派姆单抗(每3周2mg/kg)或纳武单抗(每2周3mg/kg)后1个月内开始放疗,且照射野以外至少有一处转移灶。我们使用线性二次(LQ)模型为每位患者估计ICI期间的总剂量,以10Gy的α/β表示为2Gy等效剂量(EQD2)。需要放射影像显示放疗完成前NiLs进展或无变化,放疗完成后消退。影像必须在ICI或放疗开始后至少4周获取。测量NiLs短轴和长轴最长直径的表面积。168例患者中有126例(75%)接受了ICI和放疗。53%(67/126)患者同时接受治疗,其中24例(36%)符合病灶分析条件。29%(7/24)观察到远隔效应。对每位远隔效应患者的1至6个病灶(平均=3±2)进行了分析。患者被诊断为恶性黑色素瘤(MM)(=3)、非小细胞肺癌(NSCLC)(=3)和肾细胞癌(RCC)(=1)。他们接受了1次(=1)、2次(=2)或3次(=4)放疗,平均总EQD2为120.0±37.7Gy。远隔效应患者82%的放疗采用高单次剂量。MM患者接受派姆单抗治疗,NSCLC和RCC患者接受纳武单抗治疗,平均疗程为45±35周。我们证明,29%的分析患者显示出远隔效应。应用严格的纳入标准以区分远隔效应与ICI全身效应。我们的数据表明在ICI治疗下放疗全身效应的临床存在,并可能有助于开发更广泛的癌症治疗方法。