Department of Thoracic Oncology, Thoraxklinik at University Hospital of Heidelberg, Röntgenstraße 1, 69126, Heidelberg, Germany.
Translational Lung Research Center Heidelberg TLRCH, Member of the German Center for Lung Research DZL, Im Neuenheimer Feld 156, 69120, Heidelberg, Germany.
BMC Cancer. 2019 Nov 8;19(1):1074. doi: 10.1186/s12885-019-6205-0.
Hypofractionated palliative radiotherapy for metastatic lung cancer patients is frequently used in order to ease pain, to increase bone stability, to treat local mass effects, or to prolong progression-free survival at critical sites. Recently introduced, immunotherapy for patients with non-squamous non-small cell lung carcinoma (NSCLC) has significantly improved outcome in this cohort. Preclinical and early clinical data suggest that the combination of photon radiation with programmed death-1 (PD-1) targeting immunotherapies may promote a strong and durable immune response against tumor manifestations both within and beyond radiation targets.
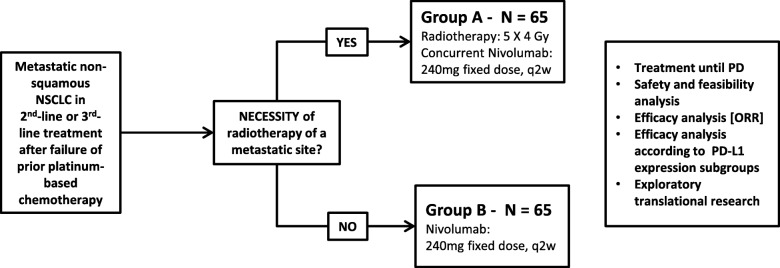
METHODS/DESIGN: In the present prospective, two-group, non-randomized, open-label phase II trial, 130 patients with stage IV non-squamous NSCLC in 2nd-line or 3rd-line treatment will be included. 65 patients with a clinical indication for palliative radiotherapy to non-cerebral/non-pulmonary metastatic sites will receive 240 mg nivolumab followed by palliative radiotherapy with 5 × 4 Gray (Gy) = 20 Gy photon radiation, which will be initiated within 72 h after first nivolumab administration (Group A). 65 patients without an indication for radiotherapy will only receive nivolumab (Group B). Nivolumab will be further administered every two weeks in both groups and will be continued until progression and loss of clinical benefit or until occurrence of limiting toxicities. The primary endpoint will be the objective response rate (ORR) according to response evaluation criteria in solid tumors (RECIST) 1.1. Secondary endpoints will be progression-free survival (PFS) according to RECIST 1.1, overall survival, descriptive subgroup analyses according to PD-L1 expression, toxicity and quality of life. Since response patterns following immunotherapies differ from those after conventional cytostatic agents, both objective response rate and progression-free survival will additionally be assessed according to immune-related RECIST (irRECIST) criteria.
The FORCE study will prospectively investigate response rates, progression-free and overall survival (OS), and toxicity of nivolumab with and without hypofractionated palliative radiotherapy in a group of 130 patients with metastatic non-small cell lung cancer (non-squamous histology) in 2nd-line or 3rd-line treatment. This trial will contribute prospective data to the repeatedly published observation that the combination of hypofractionated photon radiotherapy and medical immunotherapy is not only safe but will also promote antitumoral immune responses.
Clinicaltrials.gov identifier: NCT03044626 (Date of initial registration: 05 January 2017). Eudra-CT Number: 2015-005741-31 (Date of initial registration: 18 December 2015).
为缓解疼痛、增加骨稳定性、治疗局部肿块效应或延长关键部位无进展生存期,转移性肺癌患者常采用低分割姑息性放疗。最近,针对非鳞状非小细胞肺癌(NSCLC)患者的免疫疗法取得了显著成效。临床前和早期临床数据表明,光子放疗与程序性死亡受体-1(PD-1)靶向免疫疗法相结合,可能会在放疗靶区内外引发针对肿瘤表现的强烈和持久的免疫反应。
方法/设计:在本前瞻性、两组、非随机、开放标签的 II 期试验中,将纳入 130 例处于二线或三线治疗的 IV 期非鳞状 NSCLC 患者。65 例有姑息性放疗非脑部/非肺部转移性部位临床指征的患者将接受 240mg 纳武利尤单抗治疗,随后在首次纳武利尤单抗给药后 72 小时内接受 5×4Gy(Gy)=20Gy 光子放疗(A 组)。65 例无放疗指征的患者仅接受纳武利尤单抗治疗(B 组)。两组患者均每两周接受纳武利尤单抗治疗,并持续至疾病进展、临床获益丧失或出现限制毒性。主要终点为根据实体瘤反应评估标准(RECIST)1.1 评估的客观缓解率(ORR)。次要终点为 RECIST 1.1 评估的无进展生存期(PFS)、总生存期、根据 PD-L1 表达、毒性和生活质量进行描述性亚组分析。由于免疫治疗后的反应模式与传统细胞毒药物不同,因此根据免疫相关 RECIST(irRECIST)标准,还将评估客观缓解率和无进展生存期。
FORCE 研究将前瞻性地评估在 130 例处于二线或三线治疗的转移性非小细胞肺癌(非鳞状组织学)患者中,纳武利尤单抗联合或不联合低分割姑息性光子放疗的缓解率、无进展生存期和总生存期(OS)以及毒性。该试验将为反复发表的观察结果提供前瞻性数据,即低分割光子放疗与医学免疫治疗相结合不仅安全,而且还能促进抗肿瘤免疫反应。
Clinicaltrials.gov 标识符:NCT03044626(首次注册日期:2017 年 1 月 5 日)。Eudra-CT 编号:2015-005741-31(首次注册日期:2015 年 12 月 18 日)。