HRB Centre for Primary Care Research, Department of General Practice, Royal College of Surgeons in Ireland, Dublin, Ireland.
School of Population Health and Environmental Sciences, King's College London, London, UK.
BMJ Open. 2019 Jun 4;9(6):e024747. doi: 10.1136/bmjopen-2018-024747.
Whether unintended discontinuation of common, evidence-based, long-term medication occurs after hospitalisation; what factors are associated with unintended discontinuation; and whether the presence of documentation of medication at hospital discharge is associated with continuity of medication in general practice.
Retrospective cohort study between 2012 and 2015.
Electronic records and hospital supplied discharge notifications in 44 Irish general practices.
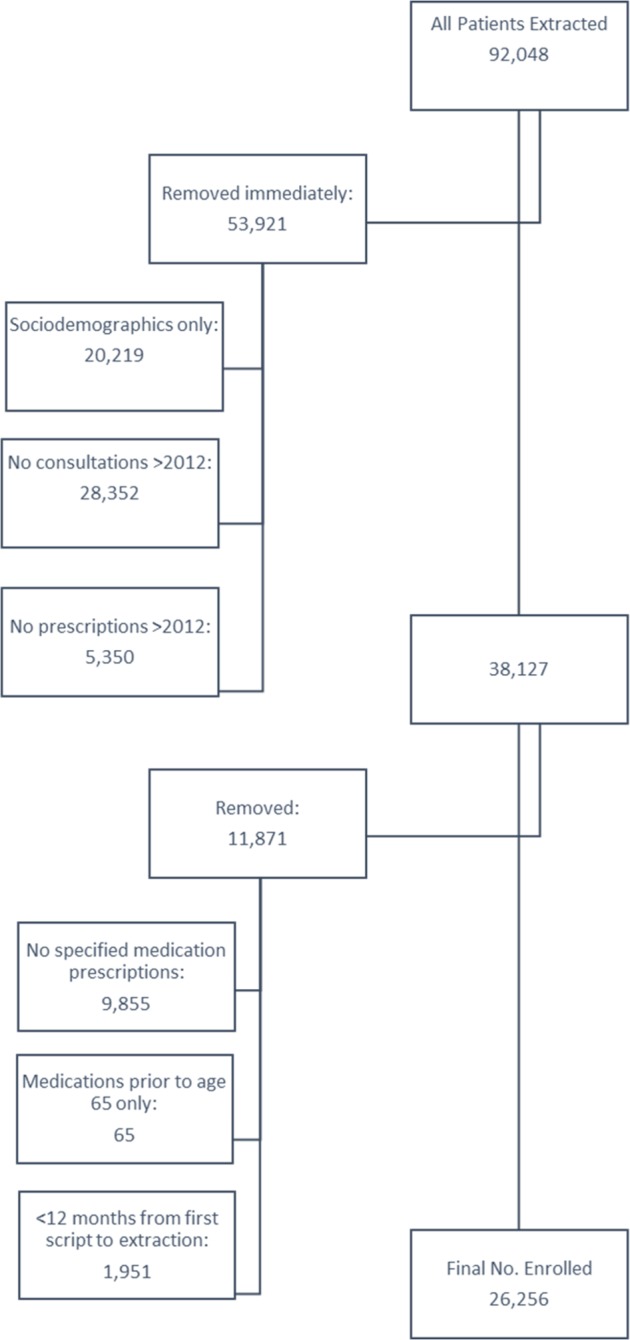
20 488 patients aged 65 years or more prescribed long-term medication for chronic conditions.
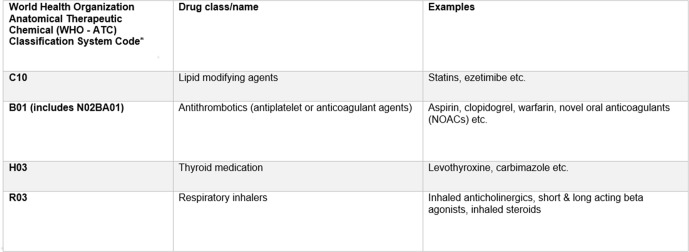
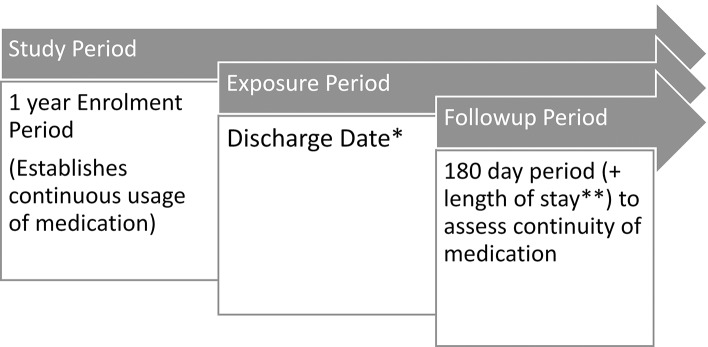
Discontinuity of four evidence-based medication drug classes: antithrombotic, lipid-lowering, thyroid replacement drugs and respiratory inhalers in hospitalised versus non-hospitalised patients; patient and health system factors associated with discontinuity; impact of the presence of medication in the hospital discharge summary on continuity of medication in a patient's general practitioner (GP) prescribing record at 6 months follow-up.
In patients admitted to hospital, medication discontinuity ranged from 6%-11% in the 6 months posthospitalisation. Discontinuity of medication is significantly lower for hospitalised patients taking respiratory inhalers (adjusted OR (AOR) 0.63, 95% CI (0.49 to 0.80), p<0.001) and thyroid medications (AOR 0.62, 95% CI (0.40 to 0.96), p=0.03). There is no association between discontinuity of medication and hospitalisation for antithrombotics (AOR 0.95, 95% CI (0.81 to 1.11), p=0.49) or lipid lowering medications (AOR 0.92, 95% CI (0.78 to 1.08), p=0.29). Older patients and those who paid to see their GP were more likely to experience increased odds of discontinuity in all four medicine groups. Less than half (39% to 47.4%) of patients had medication listed on their hospital discharge summary. Presence of medication on hospital discharge summary is significantly associated with continuity of medication in the GP prescribing record for lipid lowering medications (AOR 1.64, 95% CI (1.15 to 2.36), p=0.01) and respiratory inhalers (AOR 2.97, 95% CI (1.68 to 5.25), p<0.01).
Discontinuity of evidence-based long-term medication is common. Increasing age and private medical care are independently associated with a higher risk of medication discontinuity. Hospitalisation is not associated with discontinuity but less than half of hospitalised patients have medication recorded on their hospital discharge summary.
探讨在医院住院后是否会发生常见的、基于证据的、长期药物的意外停药;哪些因素与意外停药有关;以及医院出院小结中是否记录药物与一般实践中药物的连续性是否有关。
2012 年至 2015 年的回顾性队列研究。
44 家爱尔兰全科诊所的电子病历和医院提供的出院通知。
20488 名年龄在 65 岁或以上的患者,他们长期服用治疗慢性疾病的药物。
在住院与非住院患者中,四种基于证据的药物类别的停药情况:抗血栓形成、降脂、甲状腺替代药物和呼吸吸入器;与停药相关的患者和卫生系统因素;在 6 个月的随访中,医院出院小结中是否记录药物对患者在全科医生(GP)处方记录中药物连续性的影响。
在住院的患者中,出院后 6 个月内药物停药率为 6%-11%。使用呼吸吸入器(调整后的比值比(AOR)0.63,95%置信区间(CI)(0.49 至 0.80),p<0.001)和甲状腺药物(AOR 0.62,95%CI(0.40 至 0.96),p=0.03)的住院患者药物停药率明显较低。抗血栓形成药物(AOR 0.95,95%CI(0.81 至 1.11),p=0.49)或降脂药物(AOR 0.92,95%CI(0.78 至 1.08),p=0.29)的停药与住院之间无关联。在所有四种药物组中,年龄较大的患者和支付医疗费用的患者更有可能增加停药的几率。只有不到一半(39%至 47.4%)的患者在其医院出院小结中列出了药物。医院出院小结中列出药物与降脂药物(AOR 1.64,95%CI(1.15 至 2.36),p=0.01)和呼吸吸入器(AOR 2.97,95%CI(1.68 至 5.25),p<0.01)在 GP 处方记录中的药物连续性显著相关。
停止使用基于证据的长期药物是很常见的。年龄增长和私人医疗保健是与药物停药风险增加独立相关的因素。住院与停药无关,但不到一半的住院患者在其医院出院小结中记录了药物。