HIV Prevention Research Unit, South African Medical Research Council, 123 Jan Hofmeyr Road, Westville, Durban, KwaZulu-Natal, 3630, South Africa.
Department of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK.
BMC Infect Dis. 2019 Jun 7;19(1):500. doi: 10.1186/s12879-019-4080-6.
Fine scale geospatial analysis of HIV infection patterns can be used to facilitate geographically targeted interventions. Our objective was to use the geospatial technology to map age and time standardized HIV incidence rates over a period of 10 years to identify communities at high risk of HIV in the greater Durban area.
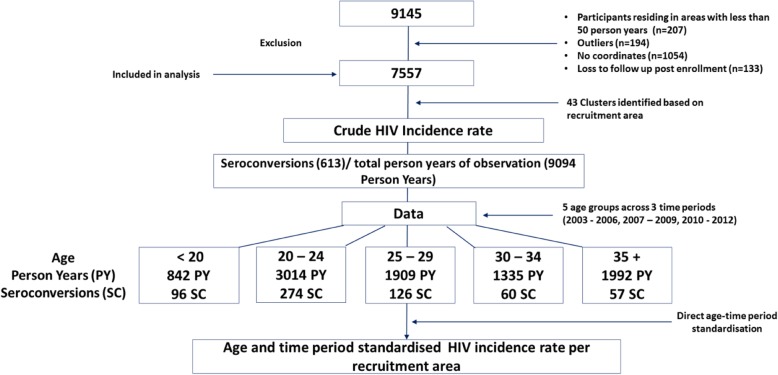
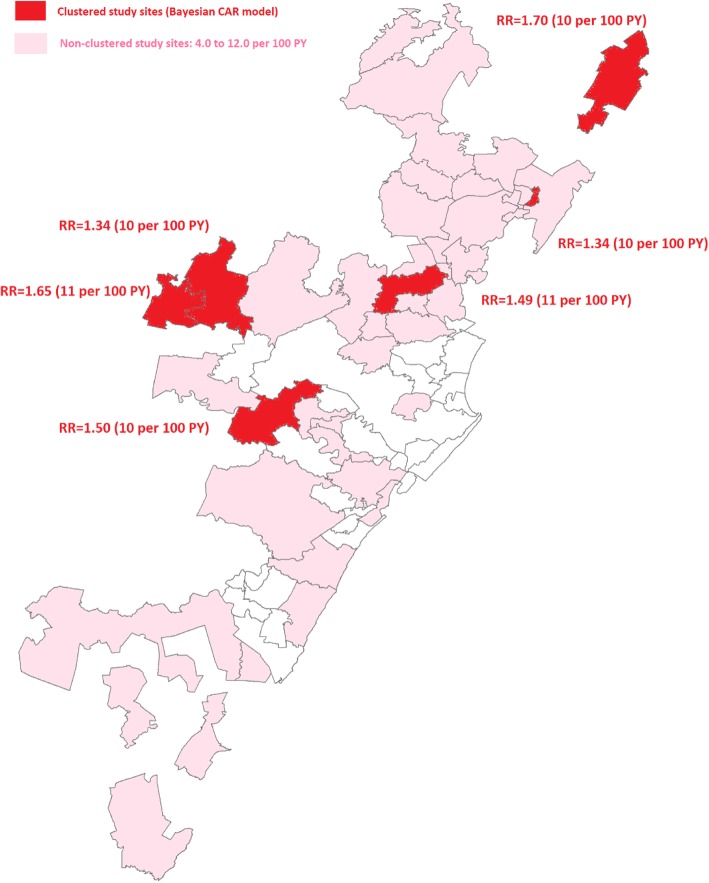
HIV incidence rates from 7557 South African women enrolled in five community-based HIV prevention trials (2002-2012) were mapped using participant household global positioning system (GPS) coordinates. Age and period standardized HIV incidence rates were calculated for 43 recruitment clusters across greater Durban. Bayesian conditional autoregressive areal spatial regression (CAR) was used to identify significant patterns and clustering of new HIV infections in recruitment communities.
The total person-time in the cohort was 9093.93 years and 613 seroconversions were observed. The overall crude HIV incidence rate across all communities was 6·74 per 100PY (95% CI: 6·22-7·30). 95% of the clusters had HIV incidence rates greater than 3 per 100PY. The CAR analysis identified six communities with significantly high HIV incidence. Estimated relative risks for these clusters ranged from 1.34 to 1.70. Consistent with these results, age standardized HIV incidence rates were also highest in these clusters and estimated to be 10 or more per 100 PY. Compared to women 35+ years old younger women were more likely to reside in the highest incidence areas (aOR: 1·51, 95% CI: 1·06-2·15; aOR: 1.59, 95% CI: 1·19-2·14 and aOR: 1·62, 95% CI: 1·2-2·18 for < 20, 20-24, 25-29 years old respectively). Partnership factors (2+ sex partners and being unmarried/not cohabiting) were also more common in the highest incidence clusters (aOR 1.48, 95% CI: 1.25-1.75 and aOR 1.54, 95% CI: 1.28-1.84 respectively).
Fine geospatial analysis showed a continuous, unrelenting, hyper HIV epidemic in most of the greater Durban region with six communities characterised by particularly high levels of HIV incidence. The results motivate for comprehensive community-based HIV prevention approaches including expanded access to PrEP. In addition, a higher concentration of HIV related services is required in the highest risk communities to effectively reach the most vulnerable populations.
对 HIV 感染模式的精细地理空间分析可用于促进有针对性的地理干预。我们的目标是利用地理空间技术,对 10 年间年龄和时间标准化的 HIV 发病率进行绘图,以确定德班大都市区高危 HIV 社区。
使用参与者家庭全球定位系统 (GPS) 坐标,对 7557 名参加五项社区为基础的 HIV 预防试验的南非女性的 HIV 发病率进行绘图(2002-2012 年)。为德班大都市区的 43 个招募集群计算年龄和时期标准化的 HIV 发病率。使用贝叶斯条件自回归面积空间回归 (CAR) 来识别新的 HIV 感染在招募社区中的显著模式和聚类。
队列中的总人数为 9093.93 人年,观察到 613 例血清转换。所有社区的总 HIV 发病率为 6.74/100PY(95%CI:6.22-7.30)。95%的集群 HIV 发病率高于 3/100PY。CAR 分析确定了六个 HIV 发病率显著升高的社区。这些集群的估计相对风险范围为 1.34 至 1.70。与这些结果一致,这些集群的年龄标准化 HIV 发病率也最高,估计为 10 或更多/100PY。与 35 岁以上的女性相比,年轻女性更有可能居住在发病率最高的地区(aOR:1.51,95%CI:1.06-2.15;aOR:1.59,95%CI:1.19-2.14 和 aOR:1.62,95%CI:1.2-2.18 分别为 <20、20-24 和 25-29 岁)。高发病率集群中也更常见的伙伴因素(2 个以上性伴侣和未婚/未同居)(aOR 1.48,95%CI:1.25-1.75 和 aOR 1.54,95%CI:1.28-1.84)。
精细的地理空间分析显示,德班大都市区的大部分地区持续存在严重的 HIV 流行,有六个社区的 HIV 发病率特别高。结果激励我们采取全面的社区为基础的 HIV 预防方法,包括扩大 PrEP 的获取。此外,需要在高风险社区集中提供更多的 HIV 相关服务,以有效接触最脆弱人群。