From the University/British Heart Foundation Centre of Research Excellence, Centre of Cardiovascular Science, University of Edinburgh, Queen's Medical Research Institute (T.E.F., A.A., P.J.G., R.K., E.C., J.W.D., N.L.M., D.J.W., N.D.).
Department of Renal Medicine, Royal Infirmary of Edinburgh (T.E.F., P.J.G., N.D.).
Hypertension. 2019 Aug;74(2):323-330. doi: 10.1161/HYPERTENSIONAHA.119.12919. Epub 2019 Jun 10.
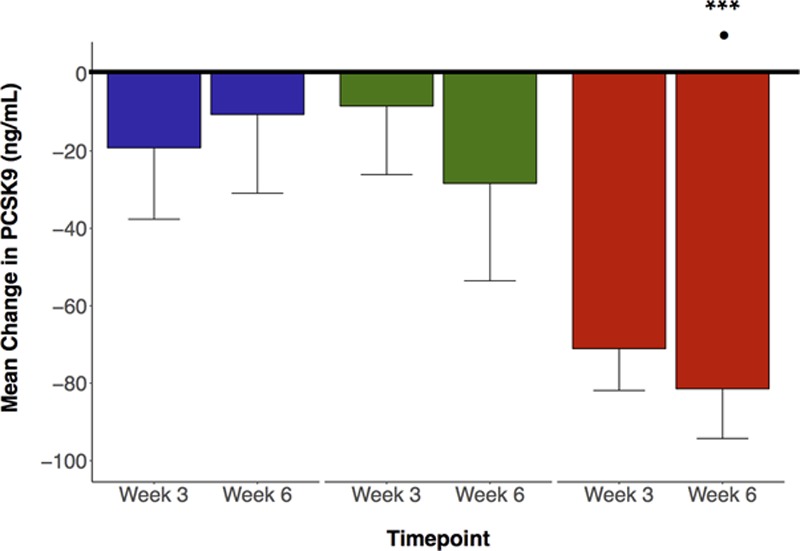
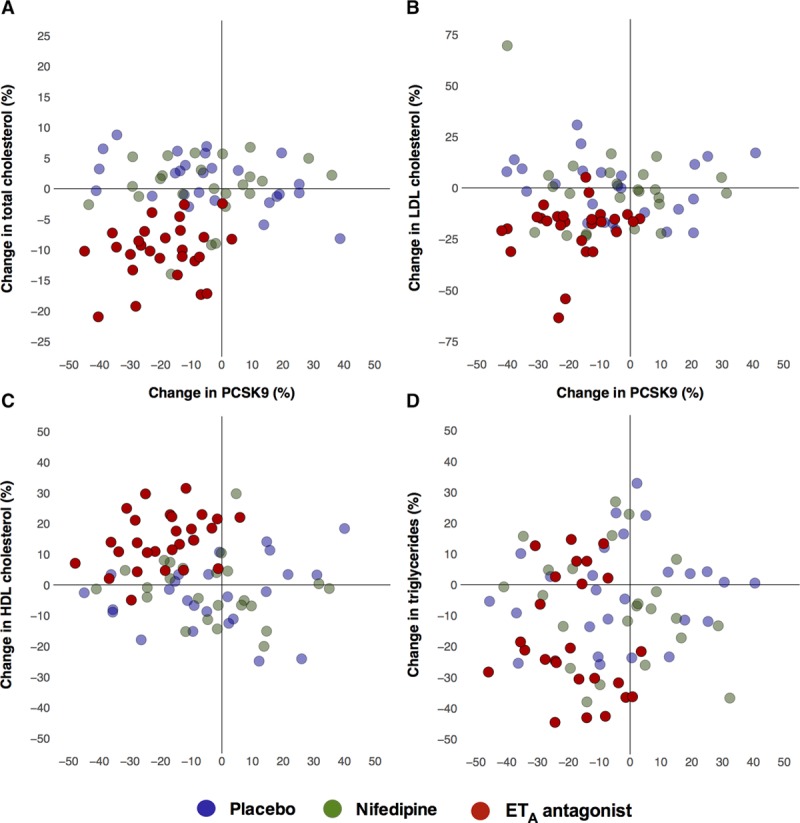
Dyslipidemia is common in chronic kidney disease (CKD). Despite statins, many patients fail to adequately lower lipids and remain at increased risk of cardiovascular disease. Selective ET (endothelin-A) receptor antagonists reduce cardiovascular disease risk factors. Preclinical data suggest that ET antagonism has beneficial effects on circulating lipids. We assessed the effects of selective ET antagonism on circulating lipids and PCSK9 (proprotein convertase subtilisin/kexin type 9) in CKD. This was a secondary analysis of a fully randomized, double-blind, 3-phase crossover study. Twenty-seven subjects with predialysis CKD on optimal cardio- and renoprotective treatment were randomly assigned to receive 6 weeks dosing with placebo, the selective ET receptor antagonist, sitaxentan, or long-acting nifedipine. We measured circulating lipids and PCSK9 at baseline and then after 3 and 6 weeks. Baseline lipids and PCSK9 did not differ before each study phase. Whereas placebo and nifedipine had no effect on lipids, 6 weeks of ET antagonism significantly reduced total (-11±1%) and low-density lipoprotein-associated (-20±3%) cholesterol, lipoprotein (a) (-16±2%) and triglycerides (-20±4%); high-density lipoprotein-associated cholesterol increased (+14±2%), P<0.05 versus baseline for all. Additionally, ET receptor antagonism, but neither placebo nor nifedipine, reduced circulating PCSK9 (-19±2%; P<0.001 versus baseline; P<0.05 versus nifedipine and placebo). These effects were independent of statin use and changes in blood pressure or proteinuria. Selective ET antagonism improves lipid profiles in optimally-managed patients with CKD, effects that may occur through a reduction in circulating PCSK9. ET receptor antagonism offers a potentially novel strategy to reduce cardiovascular disease risk in CKD. Clinical Trial Registration- URL: http://www.clinicaltrials.gov . Unique identifier: NCT00810732.
血脂异常在慢性肾脏病(CKD)中很常见。尽管使用了他汀类药物,许多患者仍未能充分降低血脂,心血管疾病风险仍然较高。选择性 ET(内皮素-A)受体拮抗剂可降低心血管疾病风险因素。临床前数据表明,ET 拮抗作用对循环脂质有有益影响。我们评估了选择性 ET 拮抗作用对 CKD 患者循环脂质和 PCSK9(前蛋白转化酶枯草溶菌素/克那霉 9)的影响。这是一项完全随机、双盲、3 期交叉研究的二次分析。27 名接受最佳心脏和肾脏保护治疗的透析前 CKD 患者被随机分配接受 6 周安慰剂、选择性 ET 受体拮抗剂西他生坦或长效硝苯地平治疗。我们在基线和 3 周和 6 周后测量循环脂质和 PCSK9。在每个研究阶段之前,基线脂质和 PCSK9 没有差异。虽然安慰剂和硝苯地平对脂质没有影响,但 ET 拮抗作用 6 周可显著降低总胆固醇(-11±1%)和低密度脂蛋白相关胆固醇(-20±3%)、脂蛋白(a)(-16±2%)和甘油三酯(-20±4%);高密度脂蛋白相关胆固醇增加(+14±2%),与基线相比所有均有统计学意义(P<0.05)。此外,ET 受体拮抗剂,而不是安慰剂或硝苯地平,降低了循环 PCSK9(-19±2%;与基线相比 P<0.001;与硝苯地平和安慰剂相比 P<0.05)。这些作用独立于他汀类药物的使用以及血压或蛋白尿的变化。选择性 ET 拮抗作用可改善最佳管理的 CKD 患者的血脂谱,其作用可能通过降低循环 PCSK9 来实现。ET 受体拮抗剂为降低 CKD 患者的心血管疾病风险提供了一种潜在的新策略。临床试验注册- 网址:http://www.clinicaltrials.gov。独特标识符:NCT00810732。