Department of Anesthesiology, Fukuoka University School of Medicine, 7-45-1, Nanakuma, Jonan-ku, Fukuoka, 814-0180, Japan.
Operation rooms, Fukuoka University Hospital, Fukuoka, Japan.
BMC Anesthesiol. 2019 Jun 15;19(1):107. doi: 10.1186/s12871-019-0780-0.
Continuous epidural infusion (CEI) has some disadvantages, such as increased local anesthetic consumption and limited area of anesthetic distribution. Programmed intermittent bolus (PIB) is a technique of epidural anesthesia in which boluses of local anesthetic are automatically injected into the epidural space. The usefulness of PIB in thoracic surgery remains unclear. In this study, we aimed to compare the efficacies of PIB epidural analgesia and CEI in patients undergoing thoracic surgery.
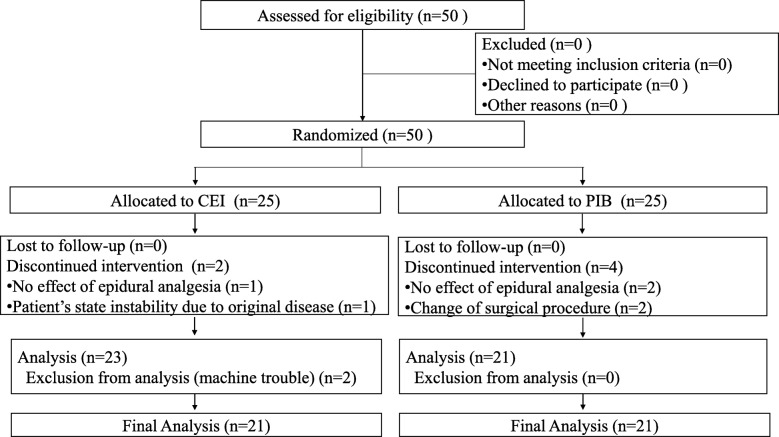
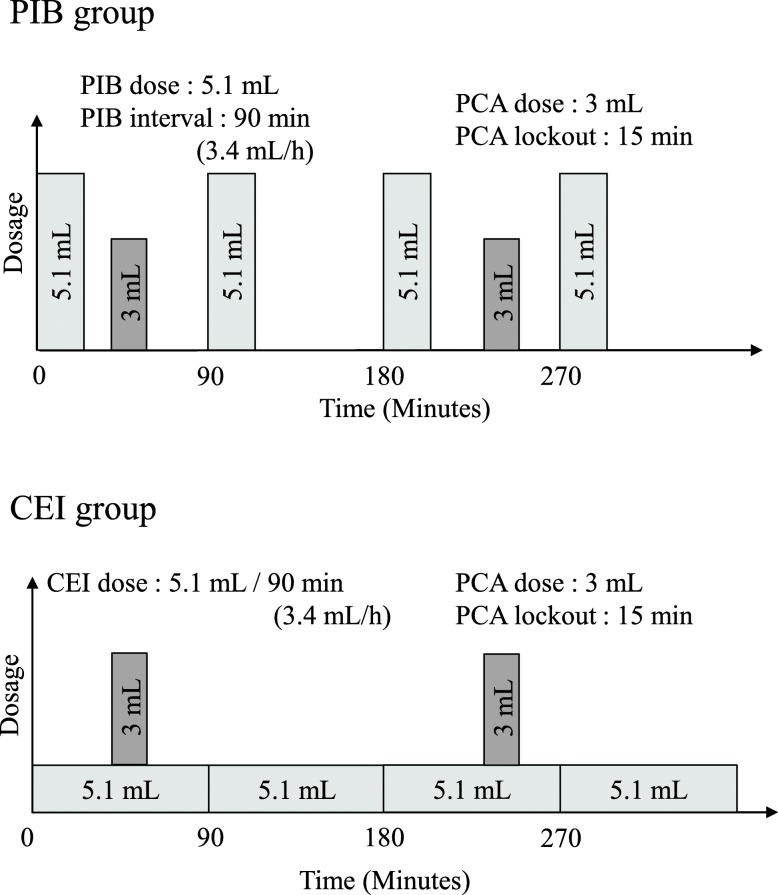
This randomized prospective study was approved by the Institutional Review Board. The study included 42 patients, who were divided into CEI (n = 21) and PIB groups (n = 21). In the CEI group, patients received continuous infusion of the local anesthetic at a rate of 5.1 mL/90 min. In the PIB group, a pump delivered the local anesthetic at a dose of 5.1 mL every 90 min. The primary endpoints were the frequency of patient-controlled analgesia (PCA) and the total dose of local anesthetic until 36 h following surgery. Student's t-test, the chi-square test, and the Mann-Whitney U test were used for statistical analyses.
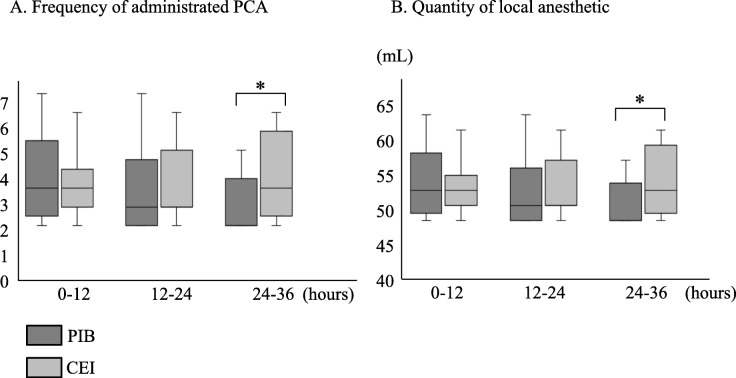
The mean number of PCA administrations and total amount of local anesthetic were not significantly different between the two groups up to 24 h following surgery. However, the mean number of PCA administrations and total amount of local anesthetic at 24-36 h after surgery were significantly lower in the PIB group than in the CEI group (median [lower-upper quartiles]: 0 [0-2.5] vs. 2 [0.5-5], P = 0.018 and 41 [41-48.5] vs. 47 [43-56], P = 0.035, respectively). Hypotension was significantly more frequent in the PIB group than in the CEI group at 0-12 h and 12-24 h (3.3% vs. 0.5%, P = 0.018 and 7.9% vs. 0%, P = 0.017, respectively).
PIB can reduce local anesthetic consumption in thoracic surgery. However, it might result in adverse events, such as hypotension.
This randomized prospective study was approved by the Institutional Review Board (IRB No. 15-9-06) of the Fukuoka University Hospital, Fukuoka, Japan, and was registered in the clinical trials database UMIN ( ID 000019904 ) on 24 November 2015. Written informed consent was obtained from all patients.
连续硬膜外输注(CEI)存在一些缺点,如局部麻醉药消耗增加和麻醉分布区域受限。程控间歇推注(PIB)是一种硬膜外麻醉技术,其中局部麻醉药以自动推注的方式注入硬膜外腔。PIB 在胸科手术中的有效性尚不清楚。本研究旨在比较 PIB 硬膜外镇痛和 CEI 在胸科手术患者中的疗效。
本随机前瞻性研究经机构审查委员会批准。研究纳入 42 例患者,分为 CEI 组(n=21)和 PIB 组(n=21)。CEI 组患者以 5.1mL/90min 的速度接受局部麻醉药持续输注。PIB 组中,泵以 5.1mL 的剂量每 90min 推注一次。主要终点为患者自控镇痛(PCA)的频率和手术结束后 36 小时内局部麻醉药的总剂量。采用 Student's t 检验、卡方检验和 Mann-Whitney U 检验进行统计学分析。
两组患者术后 24 小时内 PCA 给药次数和局部麻醉药总用量无显著差异。然而,PIB 组术后 24-36 小时 PCA 给药次数和局部麻醉药总用量明显低于 CEI 组(中位数[下四分位数-上四分位数]:0[0-2.5] vs. 2[0.5-5],P=0.018 和 41[41-48.5] vs. 47[43-56],P=0.035)。PIB 组在 0-12 小时和 12-24 小时时低血压的发生率明显高于 CEI 组(3.3% vs. 0.5%,P=0.018 和 7.9% vs. 0%,P=0.017)。
PIB 可减少胸科手术中局部麻醉药的消耗。然而,它可能导致低血压等不良事件。
本随机前瞻性研究经日本福冈大学医院机构审查委员会(IRB 编号 15-9-06)批准,并于 2015 年 11 月 24 日在 UMIN 临床试验数据库(注册号:000019904)注册。所有患者均签署了书面知情同意书。