Patkar Chinmayi Surendra, Vora Kalpana, Patel Harshal, Shah Veena, Modi Manisha Pranjal, Parikh Geeta
Department of Anaesthesia and Critical Care, G. R. Doshi and K. M. Mehta Institute of Kidney Diseases and Research Centre and Dr. H. L. Trivedi Institute of Transplantation Sciences, Civil Hospital Campus, Asarwa, Ahmedabad, Gujarat, India.
J Anaesthesiol Clin Pharmacol. 2015 Apr-Jun;31(2):234-8. doi: 10.4103/0970-9185.155155.
Minimal consumption of local anesthetic and opioid for epidural labor analgesia has been advocated for safe obstetric outcome and superior maternal satisfaction. The primary objective of this study was to evaluate and compare the analgesic efficacy of mode of administration of epidural 0.1% ropivacaine with 0.0002% fentanyl via continuous infusion or intermittent boluses during labor.
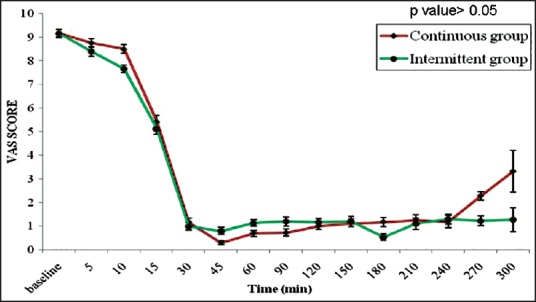
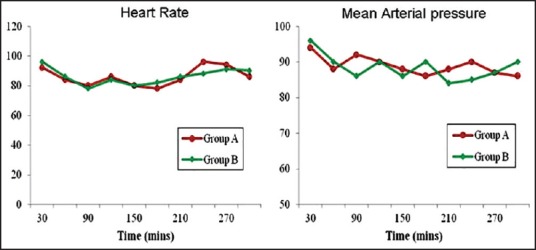
Sixty term primi or second gravida healthy parturients in labor requesting epidural analgesia were recruited in this study. Lumbar epidural catheter was inserted, and analgesia initiated with 0.2% ropivacaine. Patients were randomized to receive ropivacaine 0.1% with fentanyl 0.0002% via either continuous infusion (Group A) or intermittent boluses (Group B) on an hourly basis. If the parturient complained of pain and visual analog scale (VAS) score was >3, an additional bolus of the study drug was given. VAS score, motor blockade, maternal hemodynamics and fetal heart sounds were frequently monitored. Side effects, mode of delivery and neonatal outcome were noted.
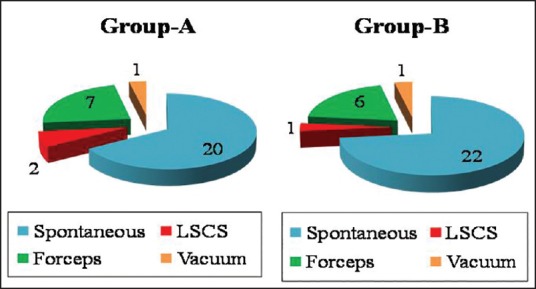
To achieve similar VAS, the mean total dose of ropivacaine was 18.78 ± 3.88 mg in Group A and 16.86 ± 4.3 mg in Group B, the difference being statistically significant (P = 0.04). Seventeen out of 30 patients in Group A that is, 56.6% and nine patients in Group B that is, 30% required additional top-ups, and this was significantly higher (P = 0.037). Side effects, mode of delivery and neonatal outcome were comparable in both groups.
Intermittent bolus administration provides a more efficacious route of drug delivery when compared to continuous infusion by significantly decreasing the total amount of local anesthetic plus opioid without adversely affecting patient safety or maternal satisfaction.
为实现安全的产科结局及更高的产妇满意度,一直提倡在硬膜外分娩镇痛中尽量减少局部麻醉药和阿片类药物的用量。本研究的主要目的是评估和比较分娩期间通过持续输注或间断推注给予硬膜外0.1%罗哌卡因与0.0002%芬太尼的镇痛效果。
本研究招募了60名足月初产妇或经产妇、正在分娩且要求硬膜外镇痛的健康产妇。插入腰段硬膜外导管,以0.2%罗哌卡因开始镇痛。患者被随机分为两组,A组通过持续输注、B组通过每小时间断推注接受0.1%罗哌卡因与0.0002%芬太尼。如果产妇主诉疼痛且视觉模拟评分(VAS)>3分,则额外给予一剂研究药物。频繁监测VAS评分、运动阻滞、产妇血流动力学及胎心音。记录副作用、分娩方式及新生儿结局。
为达到相似的VAS评分,A组罗哌卡因的平均总剂量为18.78±3.88mg,B组为16.86±4.3mg,差异有统计学意义(P=0.04)。A组30例患者中有17例(即56.6%)、B组9例患者(即30%)需要额外追加药物,A组显著更高(P=0.037)。两组的副作用、分娩方式及新生儿结局相当。
与持续输注相比,间断推注给药是一种更有效的给药途径,可显著减少局部麻醉药加阿片类药物的总量,且不会对患者安全或产妇满意度产生不利影响。