1 Institute of Applied Health Research University of Birmingham United Kingdom.
2 Department of Cardiology Chinese PLA Medical School Chinese PLA General Hospital Beijing China.
J Am Heart Assoc. 2019 Jul 2;8(13):e012546. doi: 10.1161/JAHA.119.012546. Epub 2019 Jun 25.
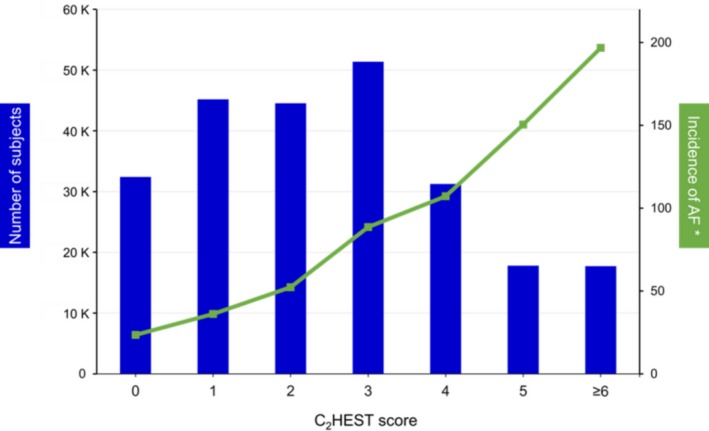
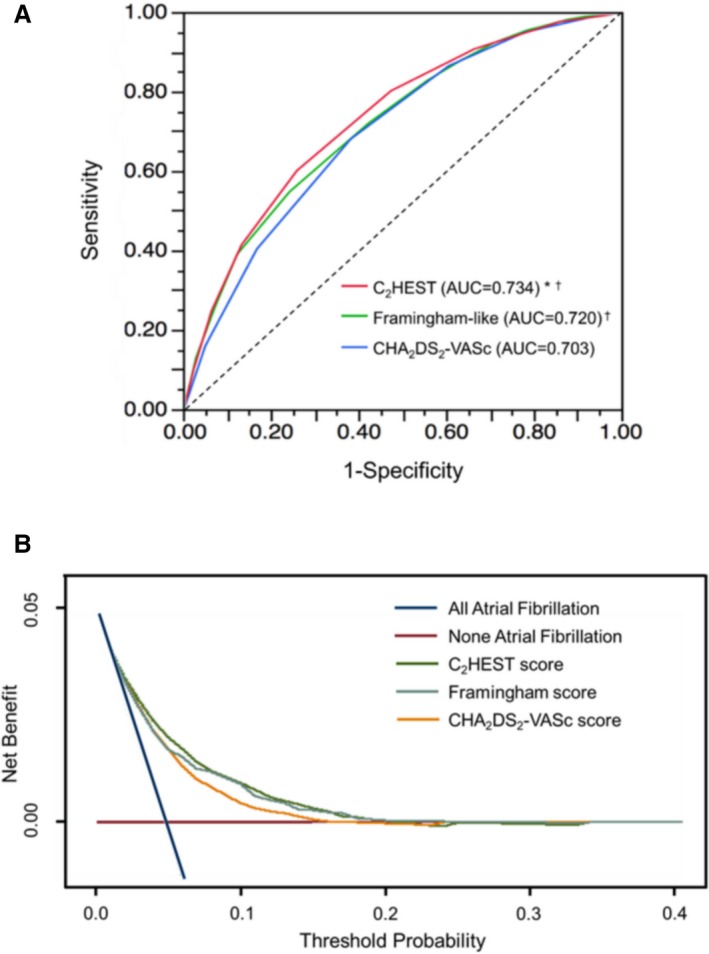
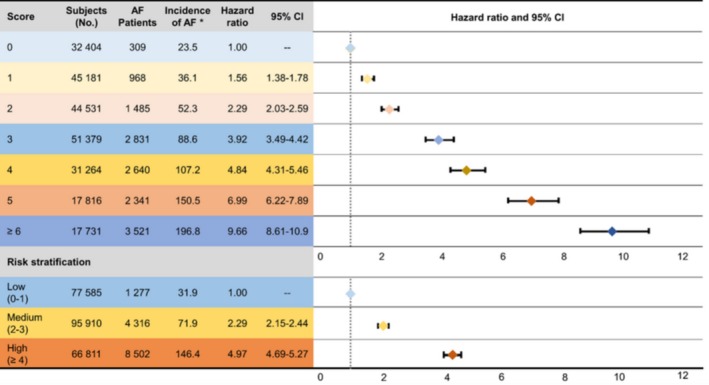
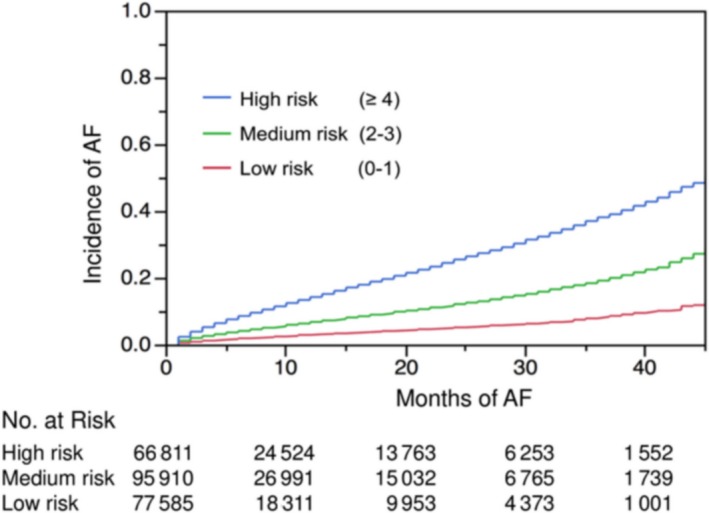
Background The CHEST score (coronary artery disease or chronic obstructive pulmonary disease [1 point each]; hypertension [1 point]; elderly [age ≥75 years, 2 points]; systolic heart failure [2 points]; thyroid disease [hyperthyroidism, 1 point]) was initially proposed for predicting incident atrial fibrillation (AF) in the general population. Its performance in poststroke patients remains to be established, especially because patients at high risk for incident AF should be targeted for more comprehensive screening. This study aimed to evaluate this newly established incident AF prediction risk score in a post-ischemic stroke population. Methods and Results Validation was based on a hospital-based nationwide cohort with 240 459 French post-ischemic stroke patients. Kaplan-Meier curves for incident rate of AF depict differences between varying risk categories. Discrimination of the CHEST score was evaluated using the C index, the net reclassification index, integrated discriminatory improvement, and decision curve analysis. During 7.9±11.5 months of follow-up, 14 095 patients developed incident AF. The incidence of AF increased from 23.5 per 1000 patient-years in patients with a CHEST score of 0 to 196.8 per 1000 patient-years in patients with a CHEST score ≥6. Kaplan-Meier curves showed a clear difference among different risk strata (log-rank P<0.0001). The CHEST score had good discrimination with a C index of 0.734 (95% CI, 0.732-0.736), which was better than the Framingham risk score and the CHADS-VASc score (congestive heart failure, hypertension, age ≥75 [doubled], diabetes mellitus, stroke [doubled], vascular disease, age 65 to 74 years, and female sex) ( P<0.0001, respectively). The CHEST score was also superior to the Framingham risk score and the CHADS-VASc score as shown by the net reclassification index, integrated discriminatory improvement ( P<0.0001, respectively) and decision curve analysis. Conclusions The CHEST score performed well in discriminating the individual risk of developing incident AF in a white European population hospitalized with previous ischemic stroke. This simple score may potentially be used as a risk stratification tool for decision making in relation to a screening strategy for AF in post-ischemic stroke patients.
CHEST 评分(冠心病或慢性阻塞性肺疾病[各 1 分];高血压[1 分];老年人[年龄≥75 岁,2 分];收缩性心力衰竭[2 分];甲状腺疾病[甲状腺功能亢进症,1 分])最初用于预测普通人群中的房颤(AF)事件。但其在缺血性卒后患者中的表现仍有待确定,尤其是因为发生 AF 风险较高的患者应进行更全面的筛查。本研究旨在评估该新建立的缺血性卒后患者房颤预测风险评分。
验证基于一项基于医院的全国性队列,其中纳入 240459 例法国缺血性卒后患者。Kaplan-Meier 曲线描述了不同风险类别之间房颤事件发生率的差异。通过 C 指数、净重新分类指数、综合区分改善和决策曲线分析评估 CHEST 评分的区分度。在 7.9±11.5 个月的随访期间,有 14095 例患者发生了房颤事件。AF 的发生率从 CHEST 评分为 0 时的每 1000 患者年 23.5 例增加到 CHEST 评分为 6 时的每 1000 患者年 196.8 例。Kaplan-Meier 曲线显示不同风险分层之间存在明显差异(log-rank P<0.0001)。CHEST 评分具有良好的区分度,C 指数为 0.734(95%CI,0.732-0.736),优于Framingham 风险评分和 CHADS-VASc 评分(充血性心力衰竭、高血压、年龄≥75 岁[加倍]、糖尿病、卒中[加倍]、血管疾病、年龄 65 至 74 岁和女性)(P<0.0001)。通过净重新分类指数、综合区分改善(P<0.0001)和决策曲线分析,CHEST 评分也优于Framingham 风险评分和 CHADS-VASc 评分。
CHEST 评分在区分白人欧洲人群缺血性卒中后住院患者发生房颤事件的个体风险方面表现良好。这种简单的评分可能可作为缺血性卒后患者房颤筛查策略中决策的风险分层工具。