MRC Biostatistics Unit, School of Clinical Medicine, University of Cambridge, Cambridge, United Kingdom.
National Infection Service, Public Health England, London, United Kingdom.
PLoS Med. 2019 Jun 27;16(6):e1002829. doi: 10.1371/journal.pmed.1002829. eCollection 2019 Jun.
Measures of the contribution of influenza to Streptococcus pneumoniae infections, both in the seasonal and pandemic setting, are needed to predict the burden of secondary bacterial infections in future pandemics to inform stockpiling. The magnitude of the interaction between these two pathogens has been difficult to quantify because both infections are mainly clinically diagnosed based on signs and symptoms; a combined viral-bacterial testing is rarely performed in routine clinical practice; and surveillance data suffer from confounding problems common to all ecological studies. We proposed a novel multivariate model for age-stratified disease incidence, incorporating contact patterns and estimating disease transmission within and across groups.
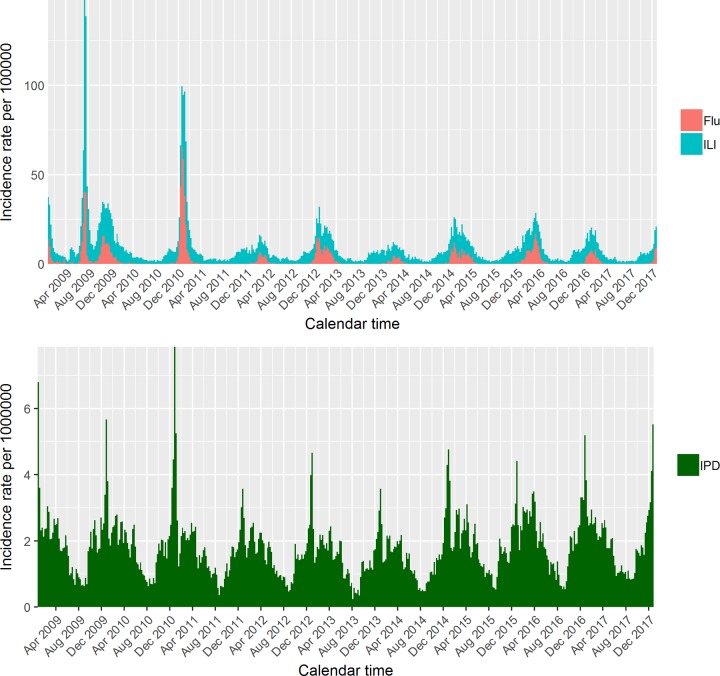
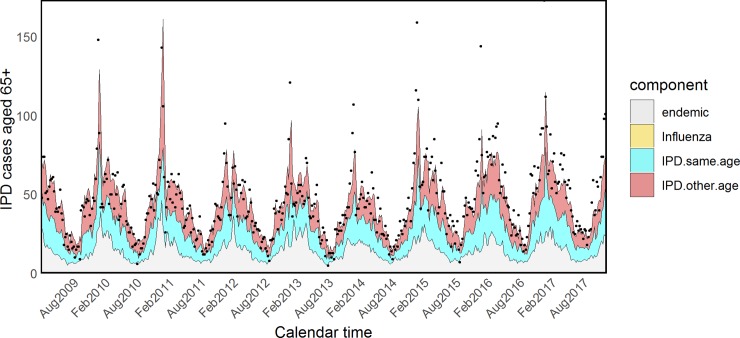
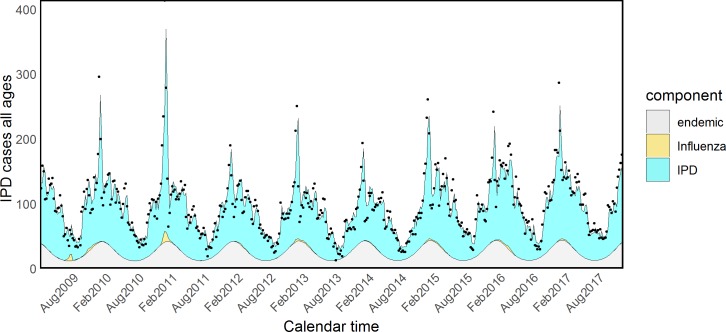
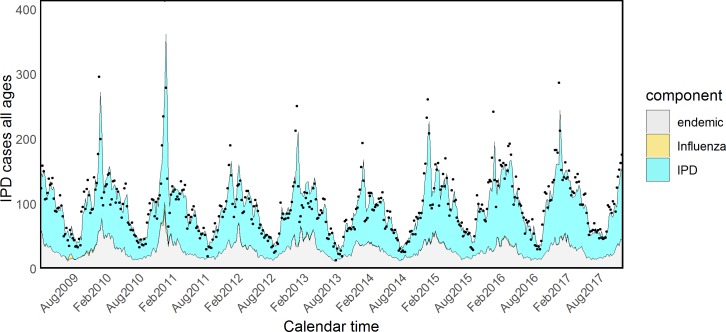
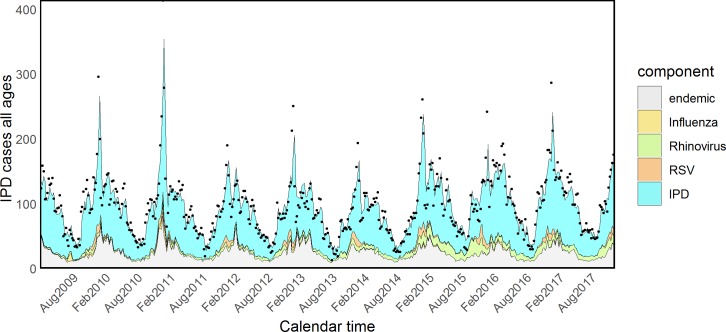
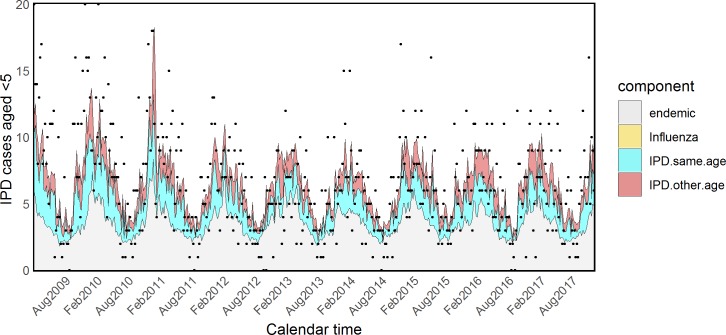
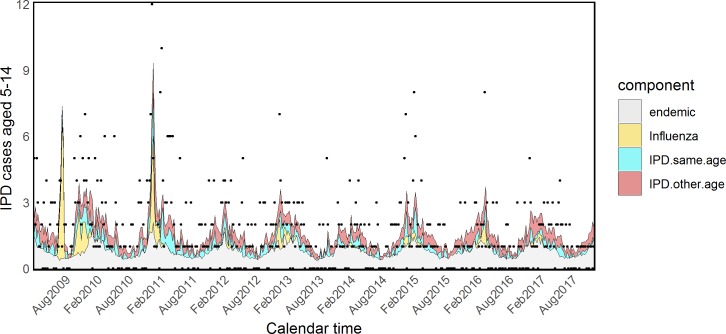
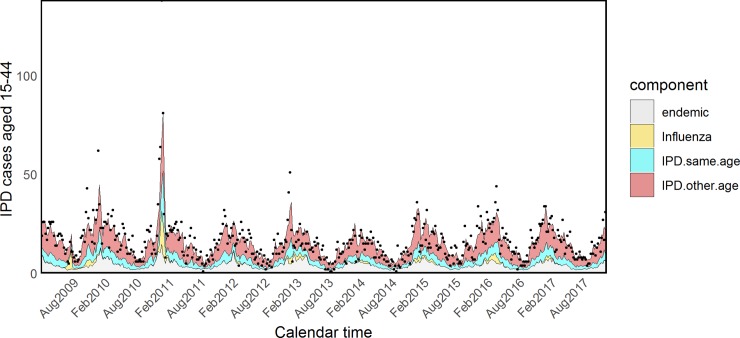
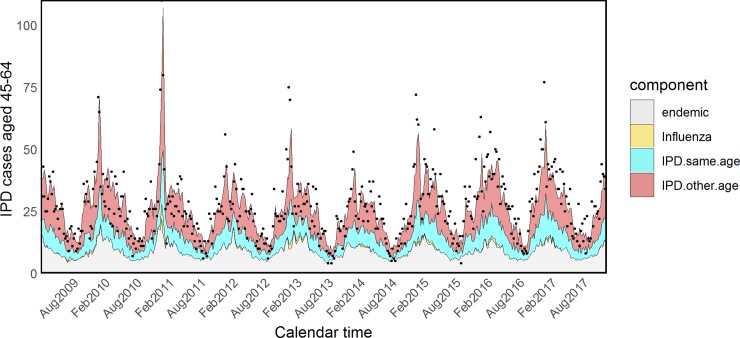
We used surveillance data from England over the years 2009 to 2017. Influenza infections were identified through the virological testing of samples taken from patients diagnosed with influenza-like illness (ILI) within the sentinel scheme run by the Royal College of General Practitioners (RCGP). Invasive pneumococcal disease (IPD) cases were routinely reported to Public Health England (PHE) by all the microbiology laboratories included in the national surveillance system. IPD counts at week t, conditional on the previous time point t-1, were assumed to be negative binomially distributed. Influenza counts were linearly included in the model for the mean IPD counts along with an endemic component describing some seasonal background and an autoregressive component mimicking pneumococcal transmission. Using age-specific counts, Akaike information criterion (AIC)-based model selection suggested that the best fit was obtained when the endemic component was expressed as a function of observed temperature and rainfall. Pneumococcal transmission within the same age group was estimated to explain 33.0% (confidence interval [CI] 24.9%-39.9%) of new cases in the elderly, whereas 50.7% (CI 38.8%-63.2%) of incidence in adults aged 15-44 years was attributed to transmission from another age group. The contribution of influenza on IPD during the 2009 pandemic also appeared to vary greatly across subgroups, being highest in school-age children and adults (18.3%, CI 9.4%-28.2%, and 6.07%, CI 2.83%-9.76%, respectively). Other viral infections, such as respiratory syncytial virus (RSV) and rhinovirus, also seemed to have an impact on IPD: RSV contributed 1.87% (CI 0.89%-3.08%) to pneumococcal infections in the 65+ group, whereas 2.14% (CI 0.87%-3.57%) of cases in the group of 45- to 64-year-olds were attributed to rhinovirus. The validity of this modelling strategy relies on the assumption that viral surveillance adequately represents the true incidence of influenza in the population, whereas the small numbers of IPD cases observed in the younger age groups led to significant uncertainty around some parameter estimates.
Our estimates suggested that a pandemic wave of influenza A/H1N1 with comparable severity to the 2009 pandemic could have a modest impact on school-age children and adults in terms of IPD and a small to negligible impact on infants and the elderly. The seasonal impact of other viruses such as RSV and rhinovirus was instead more important in the older population groups.
需要评估流感对肺炎链球菌感染的贡献程度,包括季节性和大流行背景下的贡献程度,以便预测未来大流行中继发细菌性感染的负担,为储备提供信息。由于这两种病原体的感染主要是基于症状和体征进行临床诊断,很少在常规临床实践中进行病毒-细菌联合检测,且监测数据存在所有生态学研究都存在的混杂问题,因此两者之间相互作用的程度一直难以量化。我们提出了一种新的、用于年龄分层疾病发病率的多元模型,该模型结合了接触模式,并估计了组内和组间的疾病传播。
我们使用了 2009 年至 2017 年期间英格兰的监测数据。流感感染是通过皇家全科医生学院(RCGP)运行的哨点计划中从诊断为流感样疾病(ILI)的患者中采集的样本进行病毒学检测来识别的。所有纳入国家监测系统的微生物学实验室都向英国公共卫生署(PHE)常规报告侵袭性肺炎球菌病(IPD)病例。假设 t 周的 IPD 病例数(t-1 时的条件)呈负二项分布。流感病例数与平均 IPD 病例数的季节性背景组成部分和模拟肺炎球菌传播的自回归组成部分一起线性纳入模型。使用年龄特异性计数,基于赤池信息量准则(AIC)的模型选择表明,当季节性背景组成部分表示为观察到的温度和降雨量的函数时,拟合效果最佳。同一年龄组内的肺炎球菌传播被估计为解释老年人中新病例的 33.0%(置信区间 [CI] 24.9%-39.9%),而 15-44 岁成年人中 50.7%(CI 38.8%-63.2%)的发病率归因于来自另一个年龄组的传播。2009 年大流行期间流感对 IPD 的影响似乎也因亚组而异,在学龄儿童和成年人中最高(分别为 18.3%(CI 9.4%-28.2%)和 6.07%(CI 2.83%-9.76%))。其他病毒感染,如呼吸道合胞病毒(RSV)和鼻病毒,似乎也对 IPD 有影响:RSV 导致 65+ 组中肺炎球菌感染增加 1.87%(CI 0.89%-3.08%),而 45-64 岁组中 2.14%(CI 0.87%-3.57%)的病例归因于鼻病毒。这种建模策略的有效性取决于这样一个假设,即病毒监测充分代表了人群中流感的真实发病率,而在年龄较小的组中观察到的 IPD 病例数量较少,导致一些参数估计存在较大的不确定性。
我们的估计表明,与 2009 年大流行相比,具有相当严重程度的甲型 H1N1 流感大流行可能会对学龄儿童和成年人的侵袭性肺炎球菌病产生适度影响,对婴儿和老年人的影响则较小或可忽略不计。相反,其他病毒(如 RSV 和鼻病毒)的季节性影响在年龄较大的人群中更为重要。