Ende-Verhaar Yvonne M, Ruigrok Dieuwertje, Bogaard Harm Jan, Huisman Menno V, Meijboom Lilian J, Vonk Noordegraaf Anton, Klok Frederikus A
Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, The Netherlands.
Department of Pulmonology, VU University Medical Center, Amsterdam, The Netherlands.
TH Open. 2018 Feb 27;2(1):e89-e95. doi: 10.1055/s-0038-1636537. eCollection 2018 Jan.
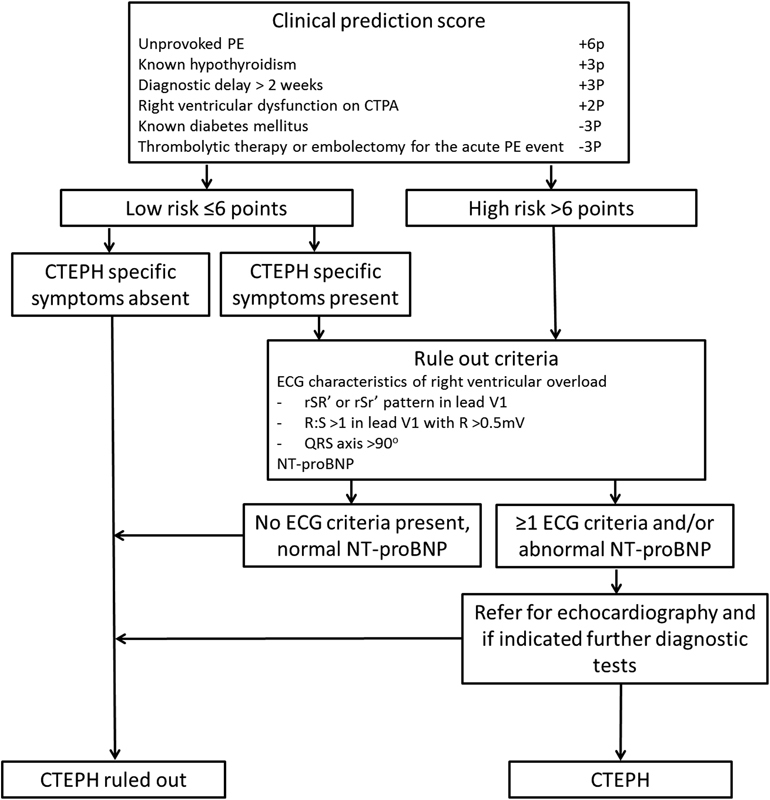
Recently, we constructed a noninvasive screening algorithm aiming at earlier chronic thromboembolic pulmonary hypertension (CTEPH) detection after acute pulmonary embolism (PE), consisting of a prediction score and combined electrocardiography (ECG)/N-terminal pro-brain natriuretic peptide (NT-proBNP) assessment. The aim of this study was to confirm the algorithm's sensitivity for CTEPH detection and to evaluate the reproducibility of its individual items. Two independent researchers calculated the prediction score in 54 consecutive patients with a history of acute PE and proven CTEPH based on clinical characteristics at PE diagnosis, and evaluated the ECG and NT-proBNP level assessed at the moment of CTEPH diagnosis. Interobserver agreement for the assessment of the prediction score, right-to-left ventricle (RV/LV) ratio measurement on computed tomography pulmonary angiography, as well as ECG reading was evaluated by calculating Cohen's kappa statistics. Median time between PE diagnosis and presentation with CTEPH was 9 months (interquartile range: 5-15). The sensitivity of the algorithm was found to be 91% (95% confidence interval [CI]: 79-97%), indicating that 27 of 30 cases of CTEPH would have been detected when applying the screening algorithm to 1,000 random PE survivors with a 3% CTEPH incidence (projected negative predictive value: 99.7%; 95% CI: 99.1-99.9%). The interobserver agreement for calculating the prediction score, RV/LV ratio measurement, and ECG reading was excellent with a kappa of 0.96, 0.95, and 0.89, respectively. The algorithm had a high sensitivity of 91% and was highly reproducible. Prospective validation of the algorithm in consecutive PE patients is required before it can be used in clinical practice.
最近,我们构建了一种无创筛查算法,旨在急性肺栓塞(PE)后更早地检测慢性血栓栓塞性肺动脉高压(CTEPH),该算法由一个预测评分以及联合心电图(ECG)/N末端脑钠肽前体(NT-proBNP)评估组成。本研究的目的是确认该算法对CTEPH检测的敏感性,并评估其各个项目的可重复性。
两名独立研究人员根据PE诊断时的临床特征,对54例有急性PE病史且经证实患有CTEPH的连续患者计算预测评分,并评估CTEPH诊断时的ECG和NT-proBNP水平。通过计算Cohen's kappa统计量来评估预测评分评估、计算机断层扫描肺动脉造影上右心室与左心室(RV/LV)比值测量以及ECG读数的观察者间一致性。
PE诊断与CTEPH出现之间的中位时间为9个月(四分位间距:5 - 15个月)。该算法的敏感性为91%(95%置信区间[CI]:79 - 97%),这表明当将筛查算法应用于1000名随机的PE幸存者(CTEPH发病率为3%)时,30例CTEPH病例中有27例将会被检测到(预计阴性预测值:99.7%;95%CI:99.1 - 99.9%)。计算预测评分、RV/LV比值测量以及ECG读数的观察者间一致性极佳,kappa值分别为0.96、0.95和0.89。
该算法具有91%的高敏感性且具有高度可重复性。在可用于临床实践之前,需要对连续的PE患者进行该算法的前瞻性验证。