Tafur Alfonso J, Fuentes Harry, Caprini Joseph A, Rivas Agustina, Uresandi F, Duce Rita, Lopez-Reyes Raquel, Visona Adriana, Merah Adel, Monreal Manuel
NorthShore University HealthSystem, Evanston, Illinois, United States.
John Stroger Cook County Hospital, Chicago, Illinois, United States.
TH Open. 2018 Apr 19;2(2):e158-e166. doi: 10.1055/s-0038-1642022. eCollection 2018 Apr.
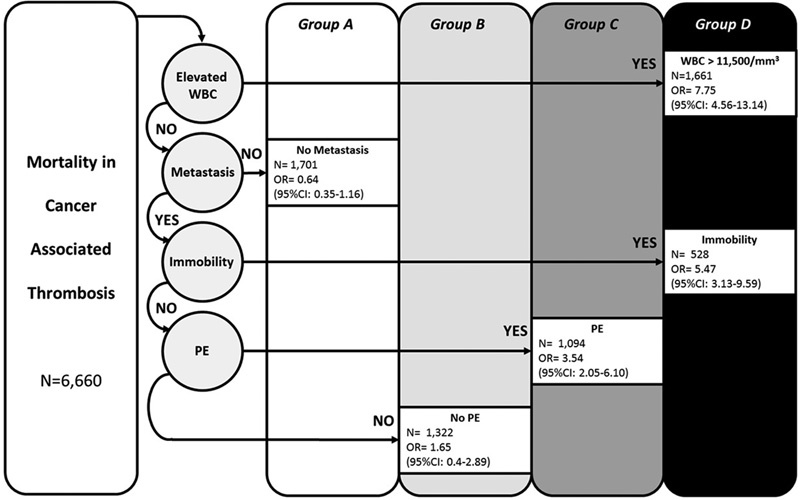
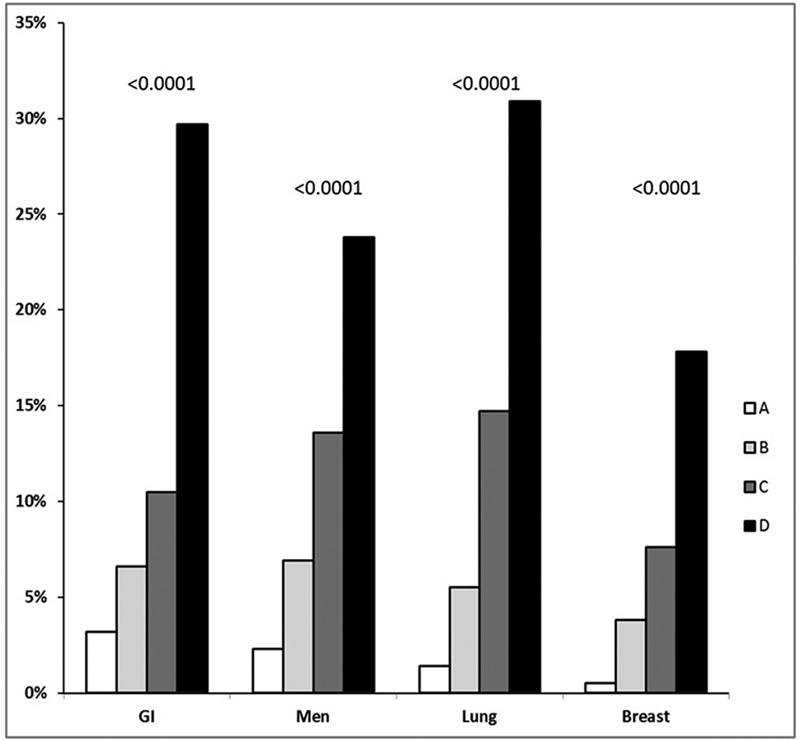
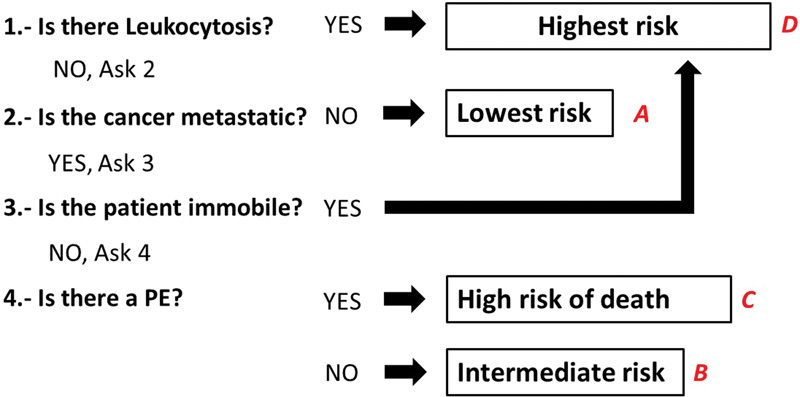
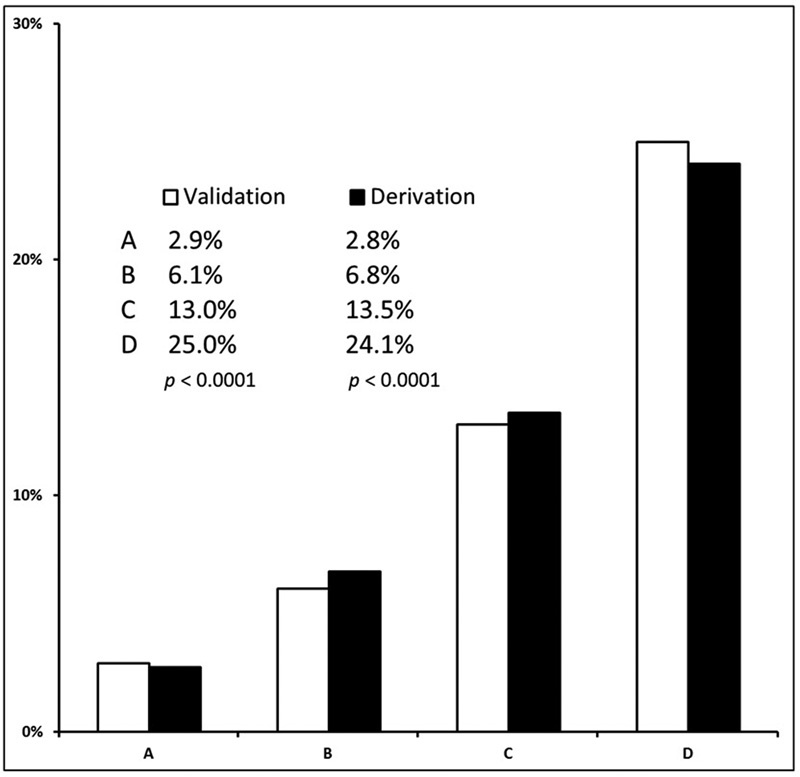
Cancer-associated thrombosis (CT) carries a high, heterogeneous, and poorly predicted likelihood of mortality. Thus, we aimed to define predictors of 30-day mortality in 10,025 patients with CT. In a randomly selected derivation cohort, we used recursive partitioning analysis to detect variables that select for a risk of mortality within 30 days. In a validation cohort, we evaluated our results using Cochran-Armitage test. The most common types of cancer were lung (16%), breast (14%), and colorectal (14%); median age was 69 years (range, 14-101); most had metastatic disease (63%); 13% of patients died within 30 days. In the derivation cohort ( = 6,660), a white blood cell (WBC) count in the highest quartile predicted early mortality (odds ratio, 7.8; 95% confidence interval [CI], 4.6-13.1); and the presence of metastatic disease, pulmonary embolism (PE), and immobility defined the risk of those with normal WBC count. We defined death risk according four sequential questions: (1) Does the patient have an elevated WBC count? (Yes, group D). (2) If no, does the patient have metastasis? (No, group A). (3) If yes, is the patient immobile? (Yes, group D). (4) If no, does the patient have a PE? (Yes, group C; no, group B). In the validation cohort ( = 3,365), the 30-day risk of death was 2.9% in group A (95% CI, 1.9-4.3), compared with 25% in group D (95% CI, 22.5-27.5), and there was a rate escalation between groups ( for trend < 0.01). In conclusion, with four sequential questions, the risk of death in CT can be easily stratified. An elevated WBC count at baseline predicted 30-day mortality better than metastases, PE, or immobility.
癌症相关血栓形成(CT)具有较高、异质性且难以预测的死亡可能性。因此,我们旨在确定10025例CT患者30天死亡率的预测因素。在一个随机选择的推导队列中,我们使用递归划分分析来检测那些提示30天内死亡风险的变量。在一个验证队列中,我们使用 Cochr an-Armitage检验来评估我们的结果。最常见的癌症类型为肺癌(16%)、乳腺癌(14%)和结直肠癌(14%);中位年龄为69岁(范围14 - 101岁);大多数患者患有转移性疾病(63%);13%的患者在30天内死亡。在推导队列(n = 6660)中,白细胞(WBC)计数处于最高四分位数可预测早期死亡(比值比,7.8;95%置信区间[CI],4.6 - 13.1);而转移性疾病、肺栓塞(PE)和活动受限则决定了白细胞计数正常患者的死亡风险。我们根据四个连续问题来定义死亡风险:(1)患者白细胞计数是否升高?(是,D组)。(2)如果否,患者是否有转移?(否,A组)。(3)如果是,患者是否活动受限?(是,D组)。(4)如果否,患者是否有PE?(是,C组;否,B组)。在验证队列(n = 3365)中,A组30天死亡风险为2.9%(95%CI,1.9 - 4.3),而D组为25%(95%CI,22.5 - 27.5),且各组之间风险呈递增趋势(趋势P < 0.01)。总之,通过四个连续问题,CT患者的死亡风险可轻松分层。基线时白细胞计数升高比转移、PE或活动受限更能预测30天死亡率。