Feng Jia-Wei, Pan Hua, Wang Lei, Ye Jing, Jiang Yong, Qu Zhen
The Third Affiliated Hospital of Soochow University, Changzhou First People's Hospital, Changzhou, China.
Front Endocrinol (Lausanne). 2019 Jun 19;10:363. doi: 10.3389/fendo.2019.00363. eCollection 2019.
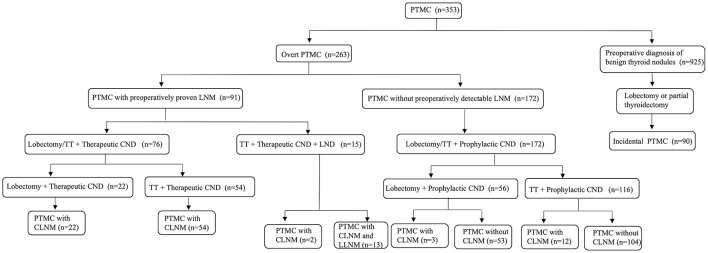
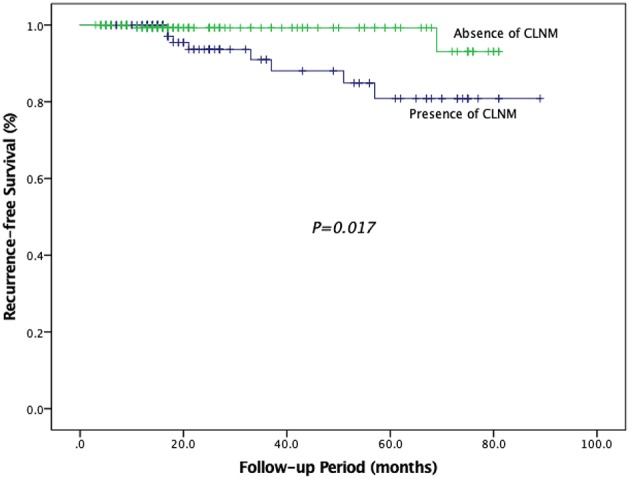
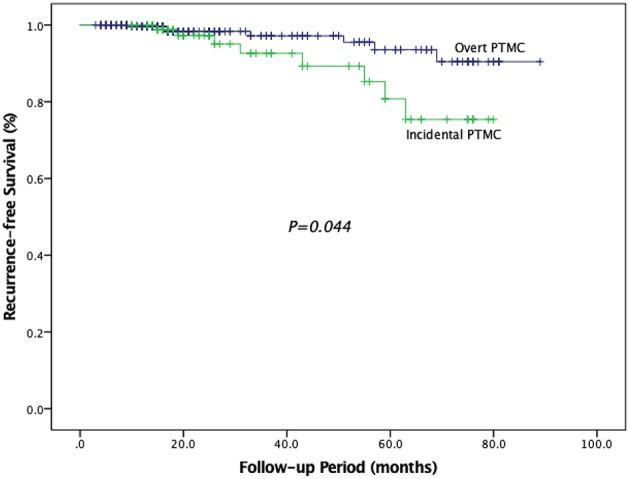
The optimal extent of surgery, including lymph node dissection, remains controversial in papillary thyroid microcarcinoma (PTMC). Determining risk factors of central lymph node metastasis (CLNM) and recurrence-free survival (RFS) may help surgeons determine individualized surgery. A total of 353 patients with PTMC were retrospectively analyzed, including 263 with overt PTMC and 90 with incidental PTMC. The recurrence rates between different extents of thyroidectomy were compared. The relationship between CLNM and clinicopathologic factors was analyzed. The Cox regression model was used to determine the risk factors for RFS. Lobectomy/total thyroidectomy (TT) with central neck dissection (CND) was performed in 263 overt PTMC patients, and lobectomy/partial thyroidectomy was performed in 90 incidental PTMC patients. In 263 overt PTMC patients, 93 (26.3%) had CLNM only and 13 (3.7%) had both CLNM and lateral lymph node metastases (LLNM). Multifocal PTMC patients who underwent lobectomy had a higher rate of thyroid bed and lymph node recurrence than patients who underwent TT ( < 0.05). Independent predictors for CLNM were age <45 years, tumor size >5 mm and presence of extrathyroidal extension (ETE). Tumor size >5 mm, multifocality, presence of ETE, presence of CLNM, and presence of LLNM were the significant factors related to the RFS. Fine-needle aspiration biopsy is advised to distinguish incidental PTMC from the benign nodules. For multifocal PTMC patients, TT should be performed to reduce recurrence. Routine prophylactic CND can be recommended in PTMC patients with independent risk factors of CLNM. Aggressive surgery and close follow-up are essential for patients with risk factors of RFS.
在甲状腺微小乳头状癌(PTMC)中,包括淋巴结清扫在内的手术最佳范围仍存在争议。确定中央淋巴结转移(CLNM)和无复发生存期(RFS)的危险因素可能有助于外科医生确定个体化手术方案。对353例PTMC患者进行回顾性分析,其中包括263例显性PTMC患者和90例偶然发现的PTMC患者。比较了不同甲状腺切除范围的复发率。分析了CLNM与临床病理因素之间的关系。采用Cox回归模型确定RFS的危险因素。263例显性PTMC患者行叶切除术/全甲状腺切除术(TT)加中央区淋巴结清扫(CND),90例偶然发现的PTMC患者行叶切除术/部分甲状腺切除术。在263例显性PTMC患者中,93例(26.3%)仅发生CLNM,13例(3.7%)同时发生CLNM和侧方淋巴结转移(LLNM)。行叶切除术的多灶性PTMC患者甲状腺床和淋巴结复发率高于行TT的患者(<0.05)。CLNM的独立预测因素为年龄<45岁、肿瘤大小>5mm和存在甲状腺外侵犯(ETE)。肿瘤大小>5mm、多灶性、存在ETE、存在CLNM和存在LLNM是与RFS相关的重要因素。建议行细针穿刺活检以区分偶然发现的PTMC与良性结节。对于多灶性PTMC患者,应行TT以降低复发率。对于具有CLNM独立危险因素的PTMC患者,可推荐常规预防性CND。对于具有RFS危险因素的患者,积极的手术和密切的随访至关重要。