Center for Rheumatology and Spine Diseases, Rigshospitalet, Valdemar Hansens vej 17, Glostrup, DK-2600, Copenhagen, Denmark.
Musculoskeletal Statistics Unit, The Parker Institute, Bispebjerg and Frederiksberg Hospital, Frederiksberg, Denmark.
Arthritis Res Ther. 2019 Jul 5;21(1):166. doi: 10.1186/s13075-019-1930-y.
To assess if the right hand, the dominant hand, or the hand with more clinically swollen joints (SwJ) is per se the most inflamed and exhibits the greatest change during treatment and hence preferred for unilateral scoring of synovitis by ultrasound in rheumatoid arthritis (RA) patients.
Using data from two previously published Norwegian RA patient cohorts initiating treatment, bilateral metacarpophalangeal joint 1-5, proximal phalangeal joint 2+3, and wrists were evaluated by ultrasound. Using a 0-3 scoring system a grey-scale (GS), power Doppler (PD) and global synovitis score (GLOESS) was calculated for each hand (0-30). For precision, a difference of < ± 3 in sum score was pre-specified as indicating clinically insignificant difference in inflammatory activity for all three scores.
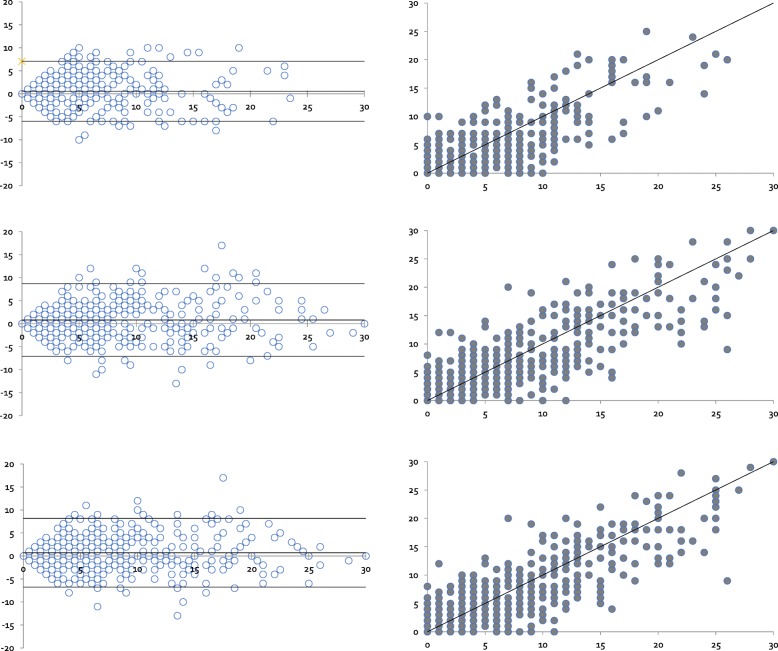
Four hundred thirty-seven RA patients were included. Baseline ultrasound inflammation was statistically significantly higher in hands with more vs fewer SwJ ([mean difference, 95%CI] GS sum score 2.21[1.30 to 3.12], PD sum score 1.70 [0.94 to 2.47] and GLOESS 2.31[1.36 to 3.26]) and also exhibited significantly more change for all sum scores at 3 months follow-up (GS sum score 1.34 [0.60 to 2.08], PD sum score 1.17 [0.44 to 1.91], and GLOESS 1.43 [0.63 to 2.22]). No such differences were found between the dominant and the non-dominant or the right and the left hands at any time points.
The hand with clinically more SwJ is statistically more inflammatory active according to GS, Doppler, and GLOESS sum scores, exhibits a change during treatment, and is potentially the best choice for unilateral scoring systems.
评估右手、优势手还是临床肿胀关节(SwJ)更多的手本身是否更具炎症性,并在治疗过程中显示出更大的变化,因此更适合用于单侧评分类风湿关节炎(RA)患者的滑膜炎。
使用来自两个先前发表的挪威 RA 患者队列的数据,对双侧掌指关节 1-5、近端指间关节 2+3 和手腕进行超声评估。使用 0-3 评分系统,对手(0-30)的每个手计算灰阶(GS)、功率多普勒(PD)和整体滑膜炎评分(GLOESS)。为了提高精度,预先规定三个评分中总分差异<±3 表示炎症活动的临床差异不显著。
共纳入 437 例 RA 患者。基线时,SwJ 较多的手的超声炎症明显高于 SwJ 较少的手([平均差异,95%CI] GS 总分 2.21[1.30 至 3.12]、PD 总分 1.70[0.94 至 2.47]和 GLOESS 2.31[1.36 至 3.26]),并且在 3 个月随访时所有总分的变化也明显更大(GS 总分 1.34[0.60 至 2.08]、PD 总分 1.17[0.44 至 1.91]和 GLOESS 1.43[0.63 至 2.22])。在任何时间点,在优势手和非优势手或右手和左手之间均未发现这种差异。
根据 GS、多普勒和 GLOESS 总分,临床 SwJ 更多的手在统计学上更具炎症活性,在治疗过程中会发生变化,因此是单侧评分系统的最佳选择。