Weller Alex, Dunlop Alex, Oxer Adam, Gunapala Ranga, Murray Iain, Gray Matthew J, Flux Glenn D, deSouza Nandita M, Ahmed Merina
1The CRUK Cancer Imaging Centre, The Institute of Cancer Research and The Royal Marsden Hospital NHS Foundation Trust, Sutton, Surrey.
2Department of Radiology, Northwick Park Hospital, Watford Road, Harrow, London.
Br J Radiol. 2019 Sep;92(1101):20190184. doi: 10.1259/bjr.20190184. Epub 2019 Jul 9.
In non-small cell lung cancer (NSCLC) patients, to establish whether the fractional volumes of irradiated anatomic or perfused lung differed between those with and without deteriorating lung function or radiation associated lung injury (RALI).
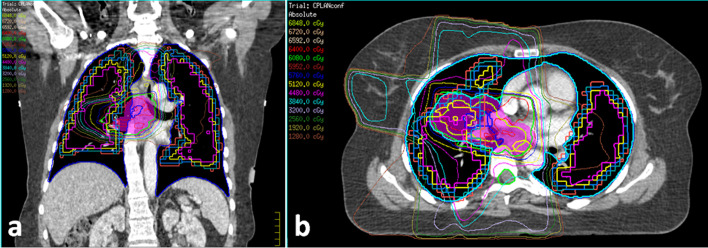
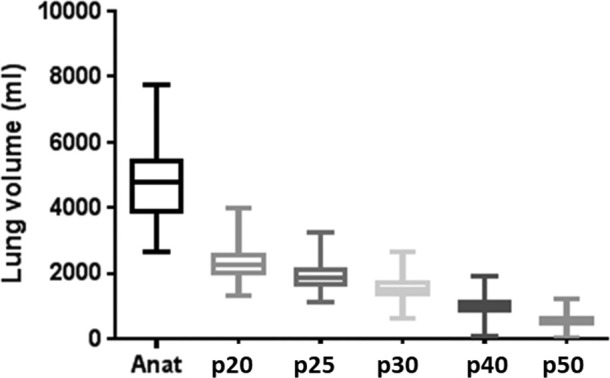
48 patients undergoing radical radiotherapy for NSCLC had a radiotherapy-planning CT scan and single photon emission CT lung perfusion imaging (Tc-labelled macroaggregate albumin). CT defined the anatomic and the single photon emission CT scan (co-registered with CT) identified the perfused (threshold 20 % of maximum) lung volumes. Fractional volumes of anatomic and perfused lung receiving more than 5, 10, 13, 20, 30, 40, 50 Gy were compared between patients with deteriorating (>median decline) stable (<median decline) forced expiratory volume in 1 s (FEV1) and between those with and without RALI (assessed by Common Toxic Criteria for Adverse Events) radiation pneumonitis and pulmonary fibrosis scores.
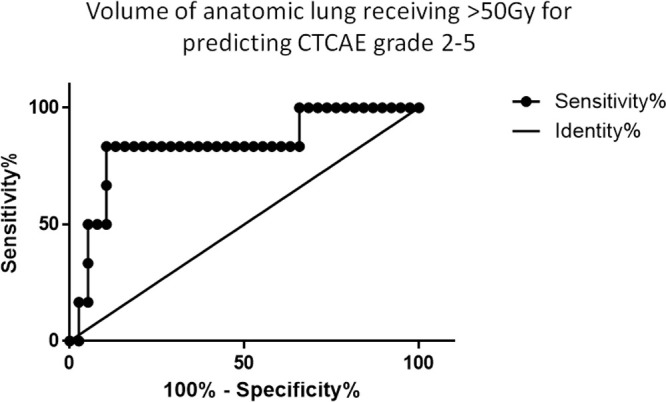
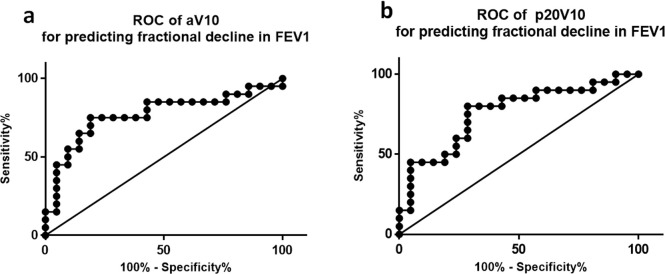
Fractional volumes of anatomic and perfused lung receiving more than 10, 13 and 20 Gy were significantly higher in patients with deteriorating stable FEV1 ( = 0.005, 0.005 and 0.025 respectively) but did not differ for higher doses of radiation (>30, 40, 50 Gy). Fractional volumes of anatomic and perfused lung receiving > 10 Gy best predicted decline in FEV1 (Area under receiver operating characteristic curve (Az = 0.77 and 0.76 respectively); sensitivity/specificity 75%/81 and 80%/71%) for a 32.7% anatomic and 33.5% perfused volume cut-off. Irradiating an anatomic fractional volume of 4.7% to > 50 Gy had a sensitivity/specificity of 83%/89 % for indicating RALI (Az = 0.83).
A 10-20 Gy radiation dose to anatomic or perfused lung results in decline in FEV1. A fractional anatomic volume of >5% receiving >50 Gy influences development of RALI.
Extent of low-dose radiation to normal lung influences functional respiratory decline.
在非小细胞肺癌(NSCLC)患者中,确定肺功能恶化或发生放射性肺损伤(RALI)与未发生者相比,受照射的解剖学肺组织或灌注肺组织的体积分数是否存在差异。
48例接受NSCLC根治性放疗的患者进行了放疗计划CT扫描和单光子发射CT肺灌注成像(锝标记的大颗粒白蛋白)。CT确定了解剖学肺组织,单光子发射CT扫描(与CT配准)确定了灌注(阈值为最大值的20%)肺组织体积。比较1秒用力呼气量(FEV1)恶化(>中位数下降)、稳定(<中位数下降)的患者以及发生和未发生RALI(根据不良事件通用毒性标准评估放射性肺炎和肺纤维化评分)的患者中,接受超过5、10、13、20、30、40、50 Gy照射的解剖学肺组织和灌注肺组织的体积分数。
FEV1恶化的患者与稳定的患者相比,接受超过10、13和20 Gy照射的解剖学肺组织和灌注肺组织的体积分数显著更高(分别为P = 0.005、0.005和0.025),但更高剂量照射(>30、40、50 Gy)时无差异。接受>10 Gy照射的解剖学肺组织和灌注肺组织的体积分数对FEV1下降的预测最佳(受试者操作特征曲线下面积(Az分别为0.77和0.76);对于32.7%的解剖学体积和33.5%的灌注体积截断值,敏感性/特异性分别为75%/81%和80%/71%)。照射4.7%的解剖学体积分数至>50 Gy对指示RALI的敏感性/特异性为83%/89%(Az = 0.83)。
对解剖学肺组织或灌注肺组织给予10 - 20 Gy的辐射剂量会导致FEV1下降。接受>50 Gy照射的解剖学体积分数>5%会影响RALI的发生。
正常肺组织低剂量辐射的范围会影响呼吸功能下降。