Department of Pulmonary Diseases, University of Groningen, University Medical Center Groningen, Hanzeplein 1, P.O. Box 30.0001, 9700, RB, Groningen, The Netherlands.
Department of Medical Cell BioPhysics, Faculty of Sciences and Technology, University of Twente, Enschede, The Netherlands.
J Immunother Cancer. 2019 Jul 10;7(1):173. doi: 10.1186/s40425-019-0649-2.
Non-small cell lung cancer (NSCLC) patients treated with checkpoint inhibitors show long lasting responses, but it is hard to predict which patients will profit from this treatment with the currently used marker, programmed death ligand 1 (PD-L1). We hypothesized that circulating tumor cells (CTC) or tumor derived extracellular vesicles (tdEV) are markers of treatment efficacy.
Patients with advanced NSCLC treated with checkpoint inhibitors were included. Blood was drawn at baseline (T0) and at 4 weeks of treatment (T1) for analysis of CTC and tdEV using CellSearch®. Tumor response was classified as partial or complete response based on the response evaluation criteria in solid tumors (RECISTv1.1) measured 4-6 weeks after start of treatment. Durable response was defined as stable disease, partial or complete response without disease progression at 6 months. Analyses were adjusted for covariables including PD-L1 expression.
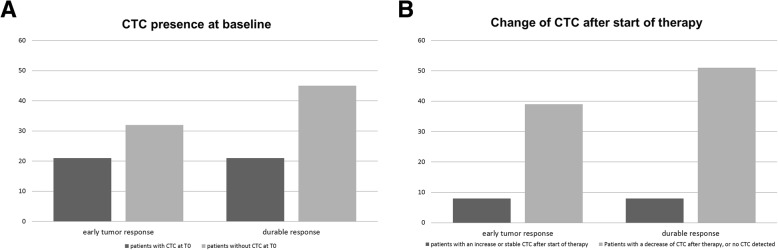
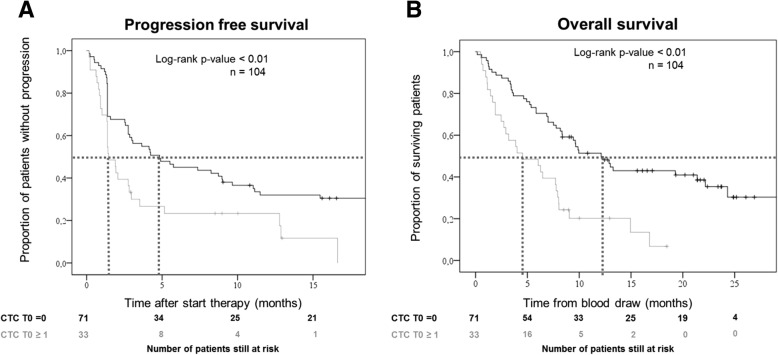
We included 104 patients (30 with a tumor response, 74 non-responders, 2 responses not evaluable due to early death); 63 patients provided T1 samples. All patients were treated with PD-L1 inhibitors. The majority of patients received second (85%) or third line (treatment with nivolumab monotherapy (89%). CTC were present in 33/104 patients at T0 (32%) and 17/63 at T1 (27%), 9/63 patients had CTC (14%) at both time points. The presence of CTC, both at T0 (OR = 0.28, p = 0.02,) and T1 (OR = 0.07, p < 0.01), was an independent predictive factor for a lack of durable response and was associated with worse progression free and overall survival. More tdEV were associated with shorter survival but not with response rate.
CTC occur in one third of advanced NSCLC patients and their presence is a predictive factor for a worse durable response rate to checkpoint inhibitors. tdEV are associated with shorter survival but not with response.
接受检查点抑制剂治疗的非小细胞肺癌(NSCLC)患者表现出持久的反应,但目前使用的程序性死亡配体 1(PD-L1)标志物很难预测哪些患者将从中受益。我们假设循环肿瘤细胞(CTC)或肿瘤衍生的细胞外囊泡(tdEV)是治疗效果的标志物。
纳入接受检查点抑制剂治疗的晚期 NSCLC 患者。在基线(T0)和治疗 4 周时(T1)采血,使用 CellSearch®分析 CTC 和 tdEV。根据治疗开始后 4-6 周的实体瘤反应评估标准(RECISTv1.1),将肿瘤反应分类为部分或完全缓解。无进展疾病定义为 6 个月时稳定疾病、部分或完全缓解且无疾病进展。分析结果针对包括 PD-L1 表达在内的协变量进行了调整。
我们纳入了 104 例患者(30 例有肿瘤反应,74 例无反应,2 例因早期死亡而无法评估反应);63 例患者提供了 T1 样本。所有患者均接受 PD-L1 抑制剂治疗。大多数患者接受二线(85%)或三线(nivolumab 单药治疗 89%)治疗。在 T0 时,33/104 例患者(32%)和 T1 时 17/63 例患者(27%)存在 CTC,63 例患者中有 9 例(14%)在两个时间点均存在 CTC。T0 时(OR=0.28,p=0.02)和 T1 时(OR=0.07,p<0.01)存在 CTC 是持久缓解缺乏的独立预测因素,与无进展生存期和总生存期更差相关。更多的 tdEV 与更短的生存时间相关,但与反应率无关。
三分之一的晚期 NSCLC 患者存在 CTC,其存在是对检查点抑制剂持久缓解率较差的预测因素。tdEV 与较短的生存时间相关,但与反应率无关。