Department of Rehabilitation, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Center, P.O. Box 9101, 6500, HB, Nijmegen, The Netherlands.
Department of Neurology and Clinical Neurophysiology, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Center, P.O. Box 9101, 6500, HB, Nijmegen, The Netherlands.
J Neuroeng Rehabil. 2019 Jul 10;16(1):86. doi: 10.1186/s12984-019-0556-2.
Peripheral changes to muscle and motor nerves occur following stroke, which may further impair functional capacity. We investigated whether a year-long use of an implanted peroneal FES system reverses stroke-related changes in muscles and motor nerves in people with foot drop in the chronic phase after supratentorial stroke.
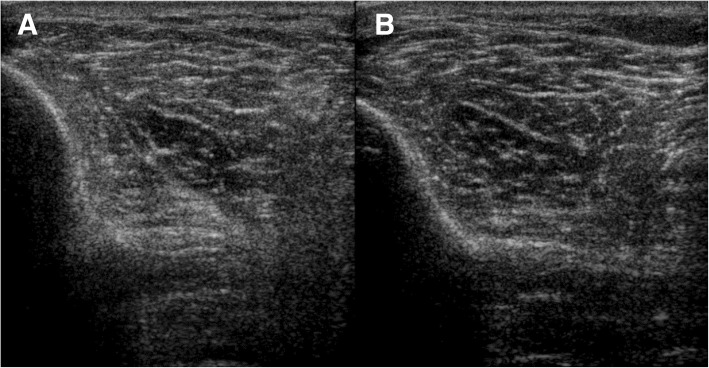
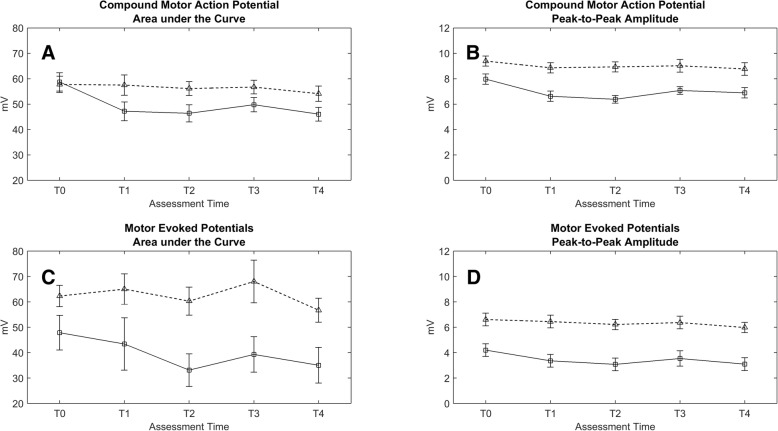
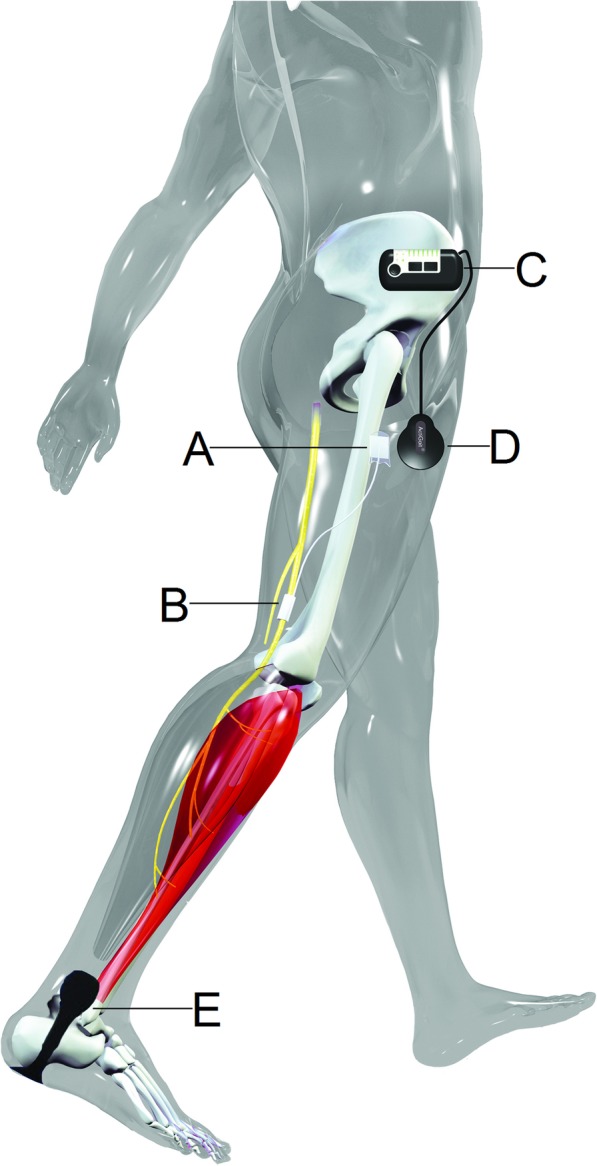
Thirteen persons with a chronic stroke (mean age 56.1 years, median Fugl-Meyer Assessment leg score 71%) were included and received an implanted peroneal FES system (ActiGait®). Quantitative muscle ultrasound (QMUS) images were obtained bilaterally from three leg muscles (i.e. tibialis anterior, rectus femoris, gastrocnemius). Echogenicity (muscle ultrasound gray value) and muscle thickness were assessed over a one-year follow-up and compared to age-, sex-, height- and weight-corrected reference values. Compound motor action potentials (CMAPs) and motor evoked potentials (MEPs) were obtained from the tibialis anterior muscle. Generalized estimated equation modeling was used to assess changes in QMUS, CMAPs and MEPs outcomes over the follow-up period.
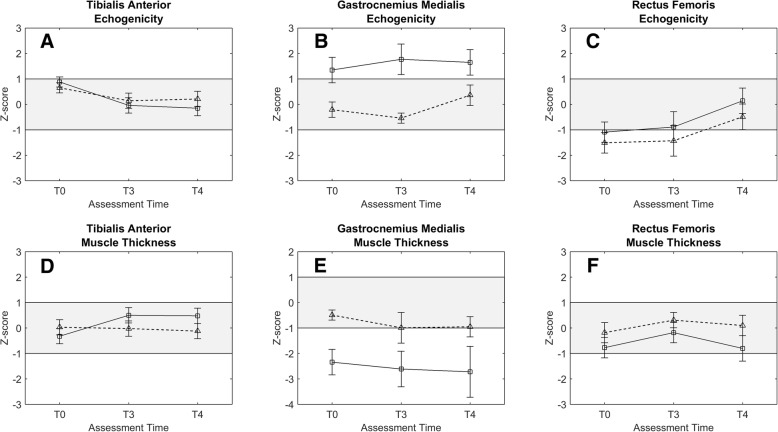
Echogenicity of the tibialis anterior decreased significantly during the follow-up on the paretic side. Z-scores changed from 0.88 at baseline to - 0.15 after 52 weeks. This was accompanied by a significant increase in muscle thickness on the paretic side, where z-scores changed from - 0.32 at baseline to 0.48 after 52 weeks. Echogenicity of the rectus femoris normalized on both the paretic and non-paretic side (z-scores changed from - 1.09 and - 1.51 to 0.14 and - 0.49, respectively). Amplitudes of CMAP and MEP (normalized to CMAP) were reduced during follow-up, particularly on the paretic side (ΔCMAP = 20% and ΔMEP = 14%).
We show that the structural changes to muscles following stroke are reversible with FES and that these changes might not be limited to electrically stimulated muscles. No evidence for improvement of the motor nerves was found.
中风后会出现肌肉和运动神经的外周变化,这可能进一步降低功能能力。我们研究了在大脑半球卒中后的慢性期,使用植入式腓肠肌 FES 系统一年是否能逆转足下垂患者的肌肉和运动神经的与中风相关的变化。
13 名慢性卒中患者(平均年龄 56.1 岁,中位数 Fugl-Meyer 评估下肢评分为 71%)接受了植入式腓肠肌 FES 系统(ActiGait®)治疗。对双侧小腿肌肉(即胫骨前肌、股直肌、腓肠肌)进行了定量肌肉超声(QMUS)成像。在一年的随访过程中,评估了肌肉回声(肌肉超声灰度值)和肌肉厚度,并与年龄、性别、身高和体重校正的参考值进行了比较。从胫骨前肌获得复合运动动作电位(CMAP)和运动诱发电位(MEP)。使用广义估计方程模型评估了随访期间 QMUS、CMAP 和 MEP 结果的变化。
在随访过程中,患侧胫骨前肌的回声显著降低。Z 评分从基线时的 0.88 降至 52 周时的-0.15。这伴随着患侧肌肉厚度的显著增加,Z 评分从基线时的-0.32 增加到 52 周时的 0.48。股直肌在患侧和非患侧均恢复正常(Z 评分分别从-1.09 和-1.51 变为 0.14 和-0.49)。CMAP 和 MEP 的振幅(与 CMAP 相比)在随访过程中降低,尤其是在患侧(ΔCMAP=20%和ΔMEP=14%)。
我们表明,FES 可逆转中风后肌肉的结构变化,并且这些变化可能不仅局限于电刺激肌肉。没有发现运动神经改善的证据。