Immunisation and Countermeasures Division, Public Health England, London, UK.
BMJ Open. 2019 Jul 11;9(7):e029087. doi: 10.1136/bmjopen-2019-029087.
To describe school-level and area-level factors that influence coverage of the school-delivered human papillomavirus (HPV) and meningococcal A, C, W and Y (MenACWY) programmes among adolescents.
Ecological study.
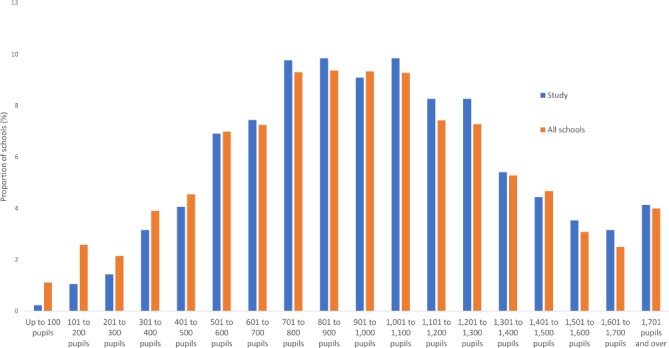
Aggregated 2016/2017 data from year 9 pupils were received from 1407 schools for HPV and 1432 schools for MenACWY. The unit of analysis was the school.
Outcome measures were percentage point (pp) difference in vaccine coverage by schools' religious affiliation, school type, urban/rural, single sex/mixed and region. A subanalysis of mixed-sex, state-funded secondary schools also included deprivation, proportion of population from black and ethnic minorities, and school size.
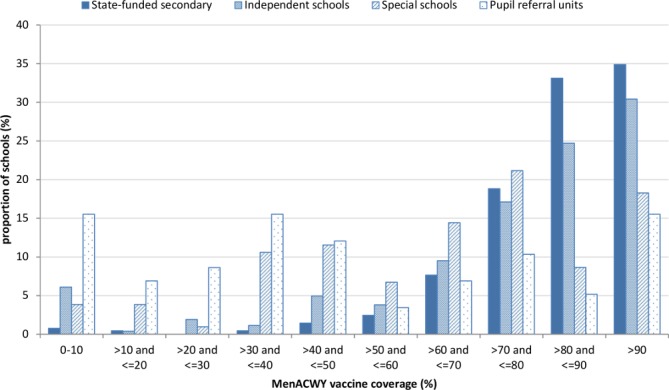
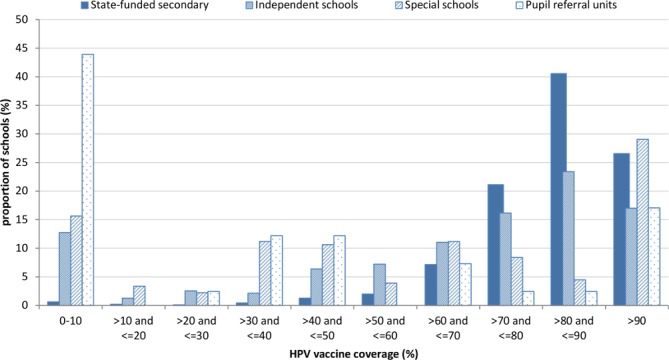
Muslim and Jewish schools had significantly lower coverage than schools of no religious character for HPV (24.0 (95% CI -38.2 to -9.8) and 20.5 (95% CI -30.7 to -10.4) pp lower, respectively) but not for MenACWY. Independent, special schools and pupil referral units had increasingly lower vaccine coverage compared with state-funded secondary schools for both HPV and MenACWY. For both vaccines, coverage was 2 pp higher in rural schools than in urban schools and lowest in London. Compared with mixed schools, HPV coverage was higher in male-only (3.7 pp, 95% CI 0.2 to 7.2) and female-only (4.8 pp, 95% CI 2 to 7.6) schools. In the subanalysis, schools located in least deprived areas had the highest coverage for both vaccines (3.8 (95% CI 0.9 to 6.8) and 10.4 (95% CI 7.0 to 13.8) pp for HPV and MenACWY, respectively), and the smallest schools had the lowest coverage (-10.4 (95% CI -14.1 to -6.8) and -7.9 (95% CI -12 to -3.8) for HPV and MenACWY, respectively).
Tailored approaches are required to improve HPV vaccine coverage in Muslim and Jewish schools. In addition, better ways of reaching pupils in smaller specialist schools are needed.
描述影响青少年学校接种人乳头瘤病毒(HPV)和脑膜炎球菌 A、C、W 和 Y(MenACWY)疫苗覆盖率的学校和地区因素。
生态研究。
从 1407 所学校(HPV 疫苗)和 1432 所学校(MenACWY 疫苗)收到了 2016/2017 年 9 年级学生的汇总数据。分析单位为学校。
疫苗接种率的结果指标是学校宗教信仰、学校类型、城乡、男女同校/混合和地区的百分点(pp)差异。男女同校、政府资助的中学的子分析还包括贫困程度、黑人和少数民族人口比例以及学校规模。
穆斯林和犹太学校的 HPV 疫苗接种率明显低于无宗教背景的学校(分别低 24.0(95%CI-38.2 至-9.8)和 20.5(95%CI-30.7 至-10.4)个百分点),但 MenACWY 疫苗接种率则不然。独立学校、特殊学校和学生转介单位的 HPV 和 MenACWY 疫苗接种率均低于政府资助的中学。对于这两种疫苗,农村学校的接种率比城市学校高 2 个百分点,而伦敦的接种率最低。与男女同校相比,HPV 疫苗接种率在仅男校(3.7 pp,95%CI 0.2 至 7.2)和仅女校(4.8 pp,95%CI 2 至 7.6)更高。在子分析中,处于最不贫困地区的学校 HPV 和 MenACWY 疫苗接种率最高(分别为 3.8(95%CI 0.9 至 6.8)和 10.4(95%CI 7.0 至 13.8)个百分点),而规模最小的学校接种率最低(HPV 和 MenACWY 分别为-10.4(95%CI-14.1 至-6.8)和-7.9(95%CI-12 至-3.8)个百分点)。
需要采取有针对性的方法来提高穆斯林和犹太学校 HPV 疫苗的接种率。此外,还需要更好的方法来接触到规模较小的专业学校的学生。