Vujovich-Dunn Cassandra, Skinner Susan Rachel, Brotherton Julia, Wand Handan, Sisnowski Jana, Lorch Rebecca, Veitch Mark, Sheppeard Vicky, Effler Paul, Gidding Heather, Venn Alison, Davies Cristyn, Hocking Jane, Whop Lisa J, Leask Julie, Canfell Karen, Sanci Lena, Smith Megan, Kang Melissa, Temple-Smith Meredith, Kidd Michael, Burns Sharyn, Selvey Linda, Meijer Dennis, Ennis Sonya, Thomson Chloe A, Lane Nikole, Kaldor John, Guy Rebecca
The Kirby Institute, University of New South Wales, Kensington, Sydney 2052, Australia.
Children's Hospital Westmead, Sydney Children's Hospitals Network, Sydney 2145, Australia.
Vaccines (Basel). 2021 Oct 19;9(10):1202. doi: 10.3390/vaccines9101202.
Australian adolescents are routinely offered HPV and dTpa (diphtheria, tetanus, pertussis) vaccines simultaneously in the secondary school vaccination program. We identified schools where HPV initiation was lower than dTpa coverage and associated school-level factors across three states.
HPV vaccination initiation rates and dTpa vaccination coverage in 2016 were calculated using vaccine databases and school enrolment data. A multivariate analysis assessed sociodemographic and school-level factors associated with HPV initiation being >5% absolute lower than dTpa coverage.
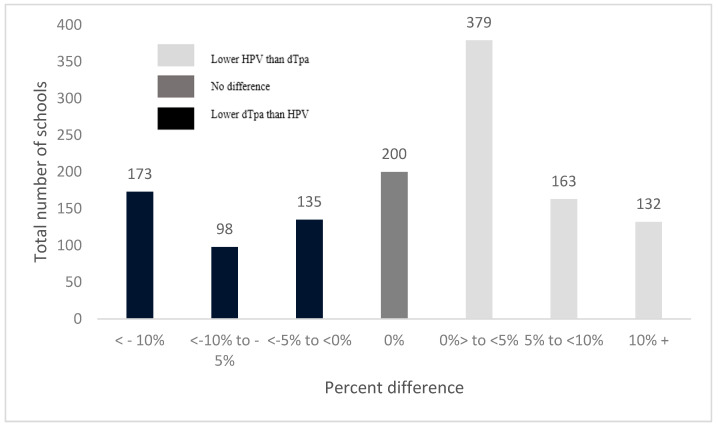
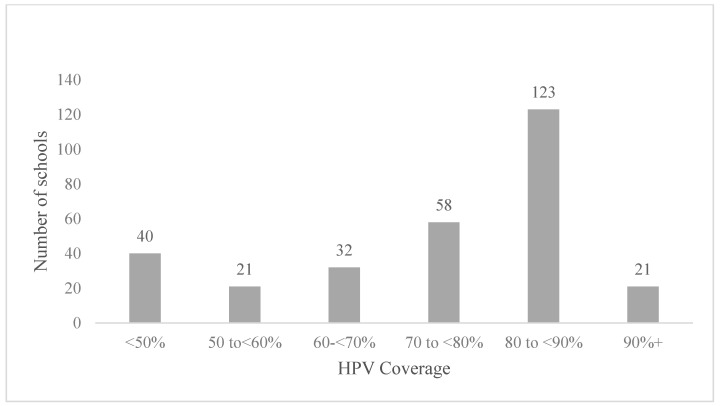
Of 1280 schools included, the median school-level HPV initiation rate was 85% (interquartile range (IQR):75-90%) and the median dTpa coverage was 86% (IQR:75-92%). Nearly a quarter (24%) of all schools had HPV vaccination initiation >5% lower than dTpa coverage and 11 % had >10% difference. School-level factors independently associated with >5% difference were remote schools (aOR:3.5, 95% CI = 1.7-7.2) and schools in major cities (aOR:1.8, 95% CI = 1.0-3.0), small schools (aOR:3.3, 95% CI = 2.3-5.7), higher socioeconomic advantage (aOR:1.7, 95% CI = 1.1-2.6), and lower proportions of Language-background-other-than-English (aOR:1.9, 95% CI = 1.2-3.0).
The results identified a quarter of schools had lower HPV than dTpa initiation coverage, which may indicate HPV vaccine hesitancy, and the difference was more likely in socioeconomically advantaged schools. As hesitancy is context specific, it is important to understand the potential drivers of hesitancy and future research needs to understand the reasons driving differential uptake.
在澳大利亚的中学疫苗接种计划中,青少年通常会同时接种人乳头瘤病毒(HPV)疫苗和白百破(dTpa,即白喉、破伤风、百日咳)疫苗。我们确定了HPV疫苗接种起始率低于dTpa疫苗接种覆盖率的学校,并分析了三个州内与之相关的学校层面因素。
利用疫苗数据库和学校入学数据计算2016年HPV疫苗接种起始率和dTpa疫苗接种覆盖率。多变量分析评估了与HPV疫苗接种起始率比dTpa疫苗接种覆盖率绝对低5%以上相关的社会人口统计学和学校层面因素。
在纳入研究的1280所学校中,学校层面HPV疫苗接种起始率的中位数为85%(四分位间距(IQR):75 - 90%),dTpa疫苗接种覆盖率的中位数为86%(IQR:75 - 92%)。近四分之一(24%)的学校HPV疫苗接种起始率比dTpa疫苗接种覆盖率低5%以上,11%的学校两者差异超过10%。与差异超过5%独立相关的学校层面因素包括偏远学校(调整后比值比(aOR):3.5,95%置信区间(CI)= 1.7 - 7.2)、大城市的学校(aOR:1.8,95% CI = 1.0 - 3.0)、小规模学校(aOR:3.3,95% CI = 2.3 - 5.7)、较高的社会经济优势(aOR:1.7,95% CI = 1.1 - 2.6)以及非英语语言背景学生比例较低(aOR:1.9,95% CI = 1.2 - 3.0)。
研究结果表明,四分之一的学校HPV疫苗接种起始率低于dTpa疫苗接种覆盖率,这可能表明存在HPV疫苗犹豫现象,且这种差异在社会经济条件较好的学校中更有可能出现。由于疫苗犹豫具有情境特异性,了解其潜在驱动因素很重要,未来的研究需要弄清楚导致不同接种率的原因。