Centre Pasteur du Cameroun, Service d'épidémiologie et de santé publique, Yaoundé, Cameroun.
Aix-Marseille Univiversité, INSERM, IRD, SESSTIM, Sciences Economiques & Sociales de la Santé & Traitement de l'Information Médicale, France.
PLoS One. 2019 Jul 18;14(7):e0219960. doi: 10.1371/journal.pone.0219960. eCollection 2019.
Long-term growth in HIV-infected infants treated early in resource-limited settings is poorly documented. Incidence of growth retardation, instantaneous risk of death related to malnutrition and growth parameters evolution during the first five years of life of uninfected and early treated HIV-infected children were compared and associated factors with growth retardation were identified.
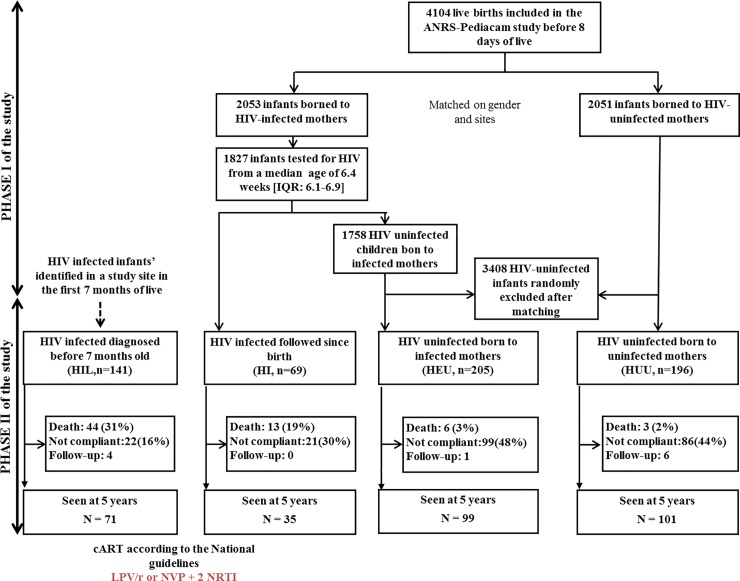
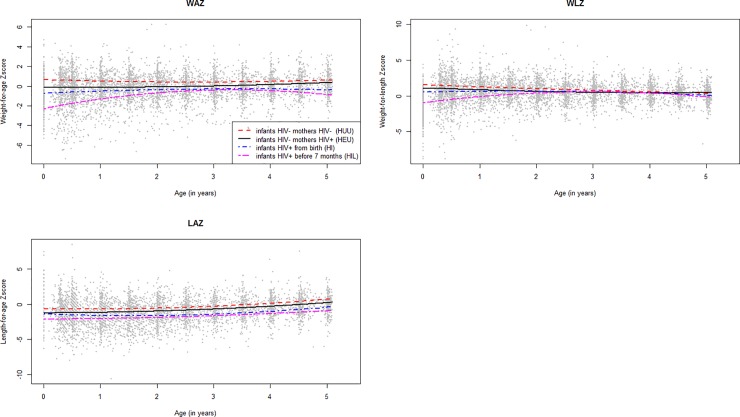
Weight-for-age (WAZ), weight-for-length (WLZ), and length-for-age (LAZ) Z-scores were calculated. The ANRS-PEDIACAM cohort includes four groups of infants with three enrolled during the first week of life: HIV-infected (HI, n = 69), HIV-exposed uninfected (HEU, n = 205) and HIV-unexposed uninfected (HUU, n = 196). The last group included HIV-infected infants diagnosed before 7 months of age (HIL, n = 141). The multi-state Markov model was used to describe the incidence of growth retardation and identified associated factors.
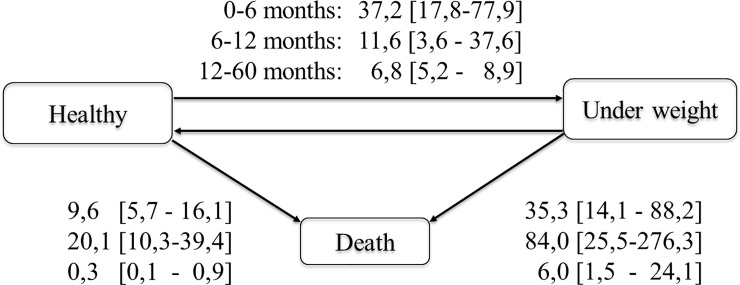
During the first 5 years, 27.5% of children experienced underweight (WAZ<-2), 60.4% stunting (LAZ<-2) and 41.1% wasting (WLZ<-2) at least once. The instantaneous risk of death observed from underweight state (35.3 [14.1-88.2], 84.0 [25.5-276.3], and 6.0 [1.5-24.1] per 1000 person-months for 0-6 months, 6-12 months, and 12-60 months respectively) was higher than from non-underweight state (9.6 [5.7-16.1], 20.1 [10.3-39.4] and 0.3 [0.1-0.9] per 1000 person-months). Compared to HEU, HIL and HI children were most at risk of wasting (adjusted HR (aHR) = 4.3 (95%CI: 1.9-9.8), P<0.001 and aHR = 3.3 (95%CI: 1.4-7.9), P = 0.01 respectively) and stunting for HIL (aHR = 8.4 (95%CI: 2.4-29.7). The risk of underweight was higher in HEU compared to HUU children (aHR = 5.0 (CI: 1.4-10.0), P = 0.001). Others associated factors to growth retardation were chronic pathologies, small size at birth, diarrhea and CD4< 25%.
HIV-infected children remained at high risk of wasting and stunting within the first 5 years period of follow-up. There is a need of identifying suitable nutritional support and best ways to integrate it with cART in pediatric HIV infection global care.
在资源有限的环境中,早期接受治疗的 HIV 感染婴儿的长期生长情况记录不佳。本研究比较了未感染和早期接受 HIV 治疗的 HIV 感染婴儿在生命的前五年中生长迟缓的发生率、与营养不良相关的即时死亡风险以及生长参数的演变,并确定了与生长迟缓相关的因素。
计算体重与年龄(WAZ)、体重与身长(WLZ)和身长与年龄(LAZ)Z 分数。ANRS-PEDIACAM 队列包括四组婴儿,其中三组在生命的第一周内入组:HIV 感染(HI,n=69)、HIV 暴露但未感染(HEU,n=205)和未感染 HIV(HUU,n=196)。最后一组包括在 7 个月龄之前被诊断为 HIV 感染的婴儿(HIL,n=141)。多状态马尔可夫模型用于描述生长迟缓的发生率并确定相关因素。
在最初的 5 年内,27.5%的儿童至少有一次体重不足(WAZ<-2),60.4%的儿童身材矮小(LAZ<-2),41.1%的儿童消瘦(WLZ<-2)。体重不足状态下观察到的即时死亡风险(0-6 个月、6-12 个月和 12-60 个月时分别为 35.3[14.1-88.2]、84.0[25.5-276.3]和 6.0[1.5-24.1]每 1000 人月)高于非体重不足状态(9.6[5.7-16.1]、20.1[10.3-39.4]和 0.3[0.1-0.9]每 1000 人月)。与 HEU 相比,HIL 和 HI 儿童最容易出现消瘦(调整后的 HR(aHR)=4.3(95%CI:1.9-9.8),P<0.001 和 aHR=3.3(95%CI:1.4-7.9),P=0.01)和 HIL 儿童的身材矮小(aHR=8.4(95%CI:2.4-29.7)。与 HUU 相比,HEU 儿童体重不足的风险更高(aHR=5.0(CI:1.4-10.0),P=0.001)。与生长迟缓相关的其他因素包括慢性疾病、出生时体重小、腹泻和 CD4<25%。
在接受 HIV 感染治疗的婴儿的前五年随访期间,仍存在较高的消瘦和身材矮小风险。需要确定合适的营养支持方法,并将其最佳方式与儿科 HIV 感染全球护理中的 cART 结合起来。