Blood and Marrow Transplant Program, University of Minnesota Medical School, Minneapolis, MN
Department of Pediatrics, University of Minnesota Medical School, Minneapolis, MN.
Haematologica. 2020 Jan 31;105(2):519-524. doi: 10.3324/haematol.2019.220970. Print 2020.
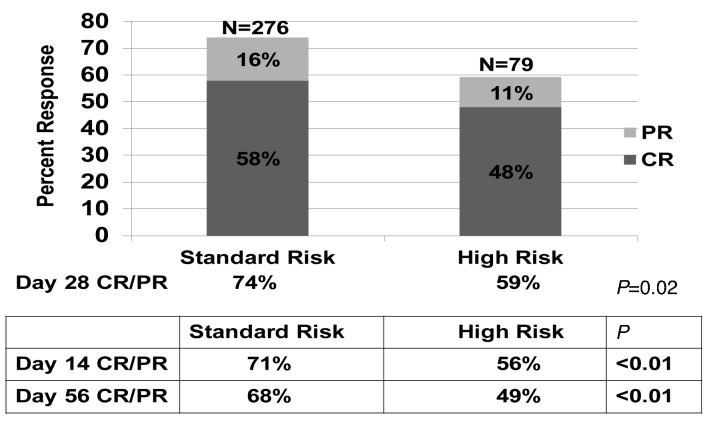
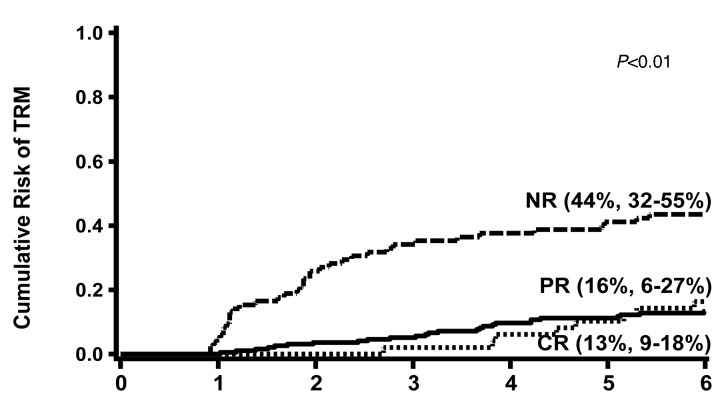
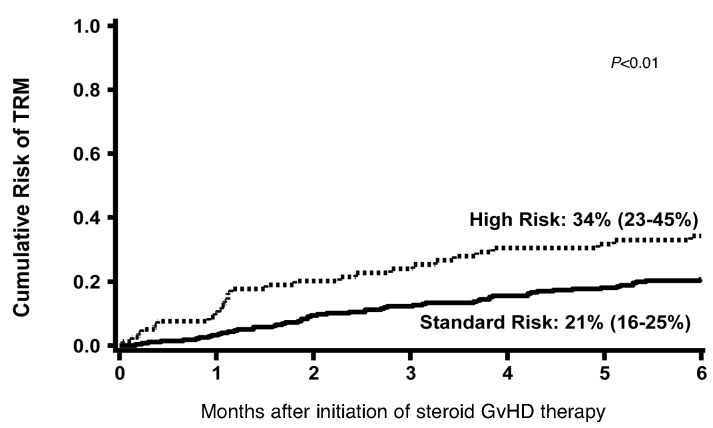
Using multicenter data, we developed a novel acute graft--host disease Risk Score which more accurately predicts response to steroid treatment, survival and transplant related mortality than other published risk scores based upon clinical grading criteria. To validate this Risk Score in a contemporary cohort, we examined 355 recent University of Minnesota patients (2007-2016) diagnosed with acute graft--host disease and treated with prednisone 60 mg/m/day for 14 days, followed by an 8-week taper. Overall response [complete response + partial response] was higher in the 276 standard risk 79 high risk graft--host disease patients at day 14 (71% 56%, <0.01), day 28 (74% versus 59%, =0.02) and day 56 (68% 49%, <0.01) after steroid initiation. Day 28 response did not differ by the initial graft--host disease grade. In multiple regression analysis, patients with high risk graft--host disease were less likely to respond at day 28 (odds ratio 0.5, 95% CI 0.3-0.9, <0.01) and had higher risks of 2 year transplant related mortality (Hazard Ratio 1.8, 95% CI, 1.0-2.1, =0.03) and overall mortality (Hazard Ratio 1.7, 95% CI, 1.2-2.4, <0.01) than patients with a standard risk graft--host disease. This analysis confirms the Minnesota graft--host disease Risk Score as a valuable bedside tool to define risk in patients with acute graft--host disease. A tailored approach to upfront acute graft--host disease therapy based upon the Minnesota Risk Score may improve outcomes and facilitate testing of novel treatments in these patients.
利用多中心数据,我们开发了一种新的急性移植物抗宿主病风险评分,与基于临床分级标准的其他已发表风险评分相比,该评分能更准确地预测对类固醇治疗的反应、存活率和与移植相关的死亡率。为了在当代队列中验证该风险评分,我们检查了 355 例最近在明尼苏达大学诊断为急性移植物抗宿主病并接受 60mg/m/天泼尼松治疗 14 天,随后进行 8 周的减量治疗的患者。在开始使用类固醇后的第 14 天(71% 比 56%,<0.01)、第 28 天(74%比 59%,=0.02)和第 56 天(68%比 49%,<0.01),标准风险(276 例)和高风险(79 例)移植物抗宿主病患者的总体反应(完全缓解+部分缓解)更高。在多变量回归分析中,高风险移植物抗宿主病患者在第 28 天的反应更差(比值比 0.5,95%CI 0.3-0.9,<0.01),且在 2 年与移植相关的死亡率(风险比 1.8,95%CI,1.0-2.1,=0.03)和总体死亡率(风险比 1.7,95%CI,1.2-2.4,<0.01)方面的风险更高,而标准风险移植物抗宿主病患者的死亡率则较低。这项分析证实了明尼苏达移植物抗宿主病风险评分是一种有价值的床边工具,可用于定义急性移植物抗宿主病患者的风险。基于明尼苏达风险评分的个体化急性移植物抗宿主病治疗方法可能会改善患者的预后,并促进对这些患者的新型治疗方法的测试。