Department of Gastroenterology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China.
Xinxiang Medical University, Xinxiang, China.
Cancer Med. 2019 Sep;8(11):5128-5136. doi: 10.1002/cam4.2431. Epub 2019 Jul 22.
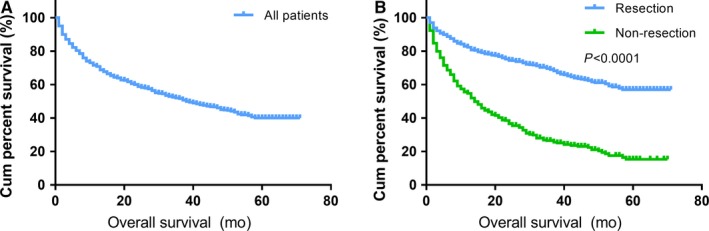
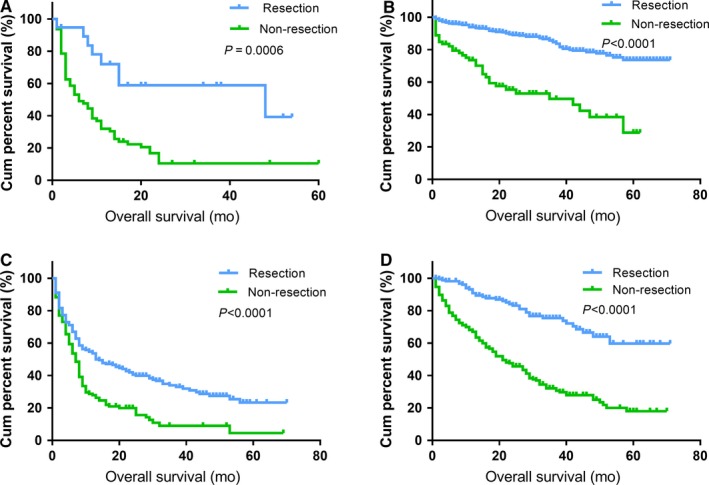
Patients who suffer from gastro-entero-pancreatic neuroendocrine neoplasms (GEP-NENs) often present with liver metastatic disease. The efficacy of primary tumor resection (PTR) for these patients remains controversial due to the relatively heterogeneous behavior of the primary tumor and the lack of clinical evidence. In this series, GEP-NEN patients with liver metastases (LM) were selected from the Surveillance, Epidemiology, and End Results database between 2010 and 2015. A logistic regression model was used to analyze variables that were associated with PTR. A Cox proportional hazards model was used to identify independent prognostic risk factors. In total, 1547 patients were enrolled in our study, including 897 patients who underwent PTR. Resection of the primary tumor was associated with prolonged survival in all patients (5-year overall survival (OS) rates: 57.0% vs 15.4%, P < .001), and improved 5-year OS rates were observed in patients with gastric, small intestinal, colorectal, and pancreatic subtypes (39.7%, 73.3%, 24.6%, and 59.7%, respectively). On the multivariate analysis, PTR was an independent prognostic factor of prolonged OS (HR = 0.48, 95% CI: 0.39-0.59, P < .001). Patients with a young age (≤60 years), small intestinal or colorectal NENs, a large primary tumor, lymph node (LN) metastases, and high tumor differentiation were more likely to undergo PTR. However, patients with colorectal NENs or a large primary tumor (≥4 cm) were at an increased risk of death independently in the PTR subgroup. The risk factors for OS also included old age, gastric tumor location, and poor differentiation. In conclusion, although PTR prolonged OS in all GEP-NEN patients presenting with LM, surgical recipients should be considered carefully. Age, primary tumor site, size, and differentiation might help surgeons identify patients who could benefit from PTR.
患有胃肠胰神经内分泌肿瘤(GEP-NENs)的患者常出现肝转移。由于原发肿瘤的行为相对异质且缺乏临床证据,因此原发肿瘤切除术(PTR)对这些患者的疗效仍存在争议。在本系列中,我们从 2010 年至 2015 年的监测、流行病学和最终结果(SEER)数据库中选择了伴有肝转移(LM)的 GEP-NEN 患者。我们使用逻辑回归模型分析与 PTR 相关的变量,并使用 Cox 比例风险模型确定独立的预后危险因素。共有 1547 名患者纳入本研究,其中 897 名患者接受了 PTR。在所有患者中,切除原发肿瘤与延长生存相关(5 年总生存率(OS)率:57.0% vs 15.4%,P<.001),并且在胃、小肠、结直肠和胰腺亚型的患者中观察到改善的 5 年 OS 率(分别为 39.7%、73.3%、24.6%和 59.7%)。多变量分析显示,PTR 是延长 OS 的独立预后因素(HR=0.48,95%CI:0.39-0.59,P<.001)。年龄≤60 岁、小肠或结直肠 NENs、较大的原发肿瘤、淋巴结(LN)转移和高肿瘤分化的患者更有可能接受 PTR。然而,在 PTR 亚组中,患有结直肠 NENs 或较大的原发肿瘤(≥4cm)的患者死亡风险独立增加。OS 的危险因素还包括年龄较大、肿瘤位于胃和分化不良。总之,尽管 PTR 延长了所有伴有 LM 的 GEP-NEN 患者的 OS,但手术接受者应仔细考虑。年龄、原发肿瘤部位、大小和分化可能有助于外科医生识别可能从 PTR 中获益的患者。