Stienen Martin Nikolaus, Geisseler Olivia, Velz Julia, Maldaner Nicolai, Sebök Martina, Dannecker Noemi, Rothacher Yannick, Schlosser Ladina, Smoll Nicolas Roydon, Keller Emanuela, Brugger Peter, Regli Luca
Department of Neurosurgery, University Hospital Zurich, University of Zurich, Zurich, Switzerland.
Clinical Neuroscience Center, University Hospital Zurich, University of Zurich, Zurich, Switzerland.
Front Neurol. 2019 Jul 3;10:734. doi: 10.3389/fneur.2019.00734. eCollection 2019.
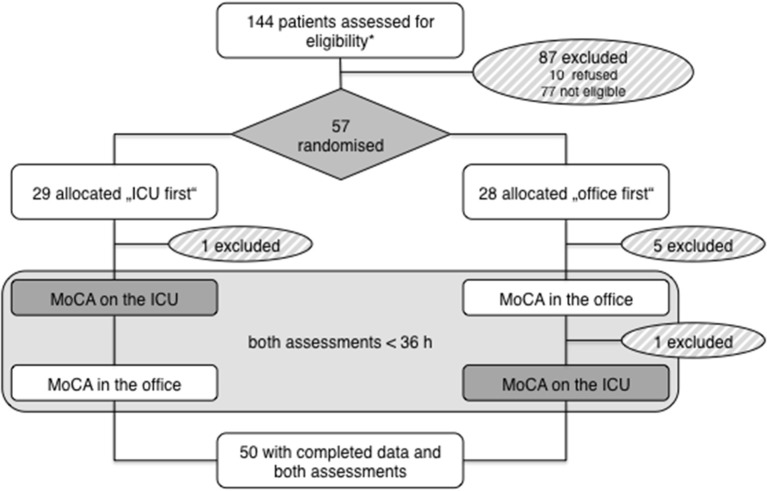
Neuropsychological screening becomes increasingly important for the evaluation of subarachnoid hemorrhage (SAH) and stroke patients. It is often performed during the surveillance period on the intensive (ICU), while it remains unknown, whether the distraction in this environment influences the results. We aimed to study the reliability of the Montreal Cognitive Assessment (MoCA) in the ICU environment. Consecutive stable patients with recent brain injury (tumor, trauma, stroke, etc.) were evaluated twice within 36 h using official parallel versions of the MoCA (ΔMoCA). The sequence of assessment was randomized into (a) busy ICU first or (b) quiet office first with subsequent crossover. For repeated MoCA, we determined sequence, period, location effects, and the intraclass correlation coefficient (ICC). = 50 patients were studied [ = 30 (60%) male], with a mean age of 57 years. The assessment's sequence ["ICU first" mean ΔMoCA -1.14 (SD 2.34) vs. "Office first" -0.73 (SD 1.52)] did not influence the MoCA ( = 0.47). On the 2nd period, participants scored 0.96 points worse (SD 2.01; = 0.001), indicating no MoCA learning effect but a possible difference in parallel versions. There was no location effect ( = 0.31) with ΔMoCA between locations (Office minus ICU) of -0.32 (SD 2.21). The ICC for repeated MoCA was 0.87 (95% CI 0.79-0.92). The reliability of the MoCA was excellent, independent from the testing environment being ICU or office. This finding is helpful for patient care and studies investigating the effect of a therapeutic intervention on the neuropsychological outcome after SAH, stroke or traumatic brain injury.
神经心理学筛查对于蛛网膜下腔出血(SAH)和中风患者的评估变得越来越重要。它通常在重症监护病房(ICU)的监测期间进行,然而,这种环境中的干扰是否会影响结果尚不清楚。我们旨在研究蒙特利尔认知评估量表(MoCA)在ICU环境中的可靠性。对近期有脑损伤(肿瘤、创伤、中风等)的连续稳定患者在36小时内使用MoCA的官方平行版本进行两次评估(ΔMoCA)。评估顺序随机分为(a)先在繁忙的ICU进行或(b)先在安静的办公室进行,随后交叉。对于重复的MoCA评估,我们确定了顺序、时期、地点效应以及组内相关系数(ICC)。共研究了50例患者[30例(60%)为男性],平均年龄57岁。评估顺序["先在ICU进行",平均ΔMoCA为-1.14(标准差2.34),而"先在办公室进行"为-0.73(标准差1.52)]对MoCA没有影响(P = 0.47)。在第二个时期,参与者得分低0.96分(标准差2.01;P = 0.001),这表明没有MoCA学习效应,但平行版本之间可能存在差异。地点之间(办公室减去ICU)的ΔMoCA没有地点效应(P = 0.31),为-0.32(标准差2.21)。重复MoCA的ICC为0.87(95%可信区间0.79 - 0.92)。MoCA的可靠性非常好,与测试环境是ICU还是办公室无关。这一发现有助于患者护理以及研究治疗干预对SAH、中风或创伤性脑损伤后神经心理结果的影响。