Zhao Mengnan, Lu Tao, Huang Yiwei, Yin Jiacheng, Jiang Tian, Li Ming, Yang Xinyu, Zhan Cheng, Feng Mingxiang, Wang Qun
Department of Thoracic Surgery, Zhongshan Hospital, Fudan University, Shanghai, China.
Eight-Year Program Clinical Medicine, Grade of 2014, Shanghai Medical College, Fudan University, Shanghai, China.
Front Oncol. 2019 Jul 3;9:593. doi: 10.3389/fonc.2019.00593. eCollection 2019.
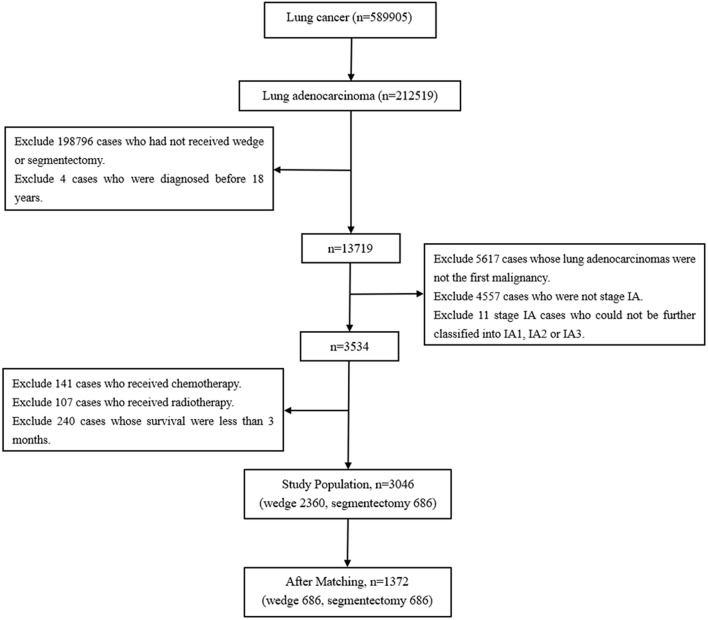
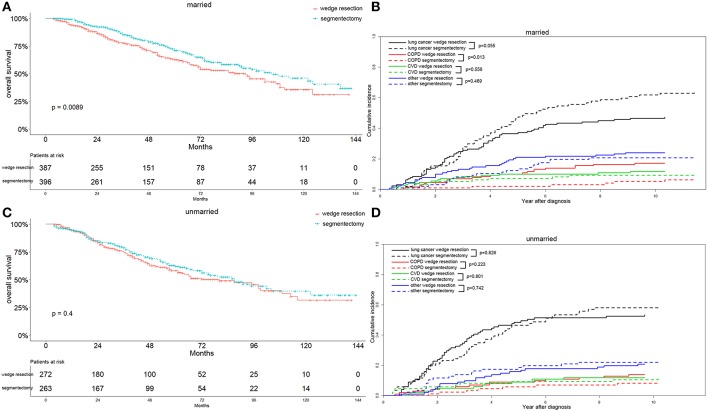
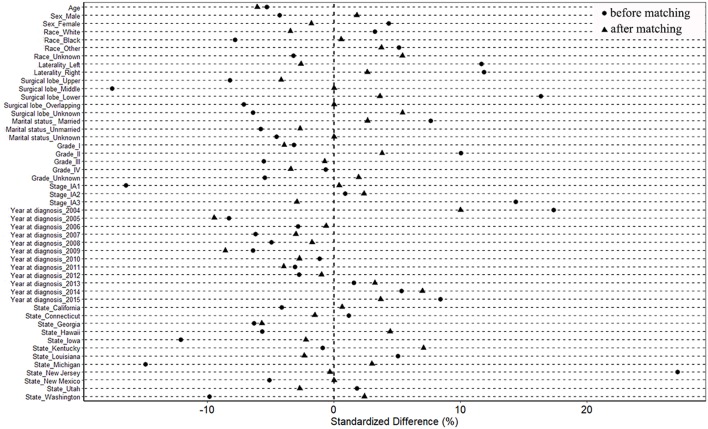
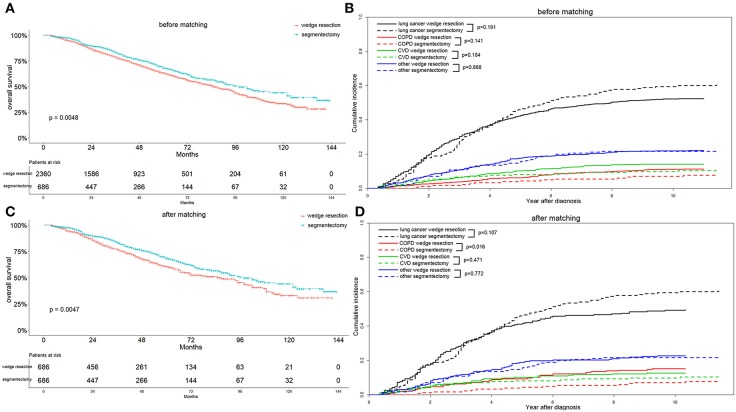
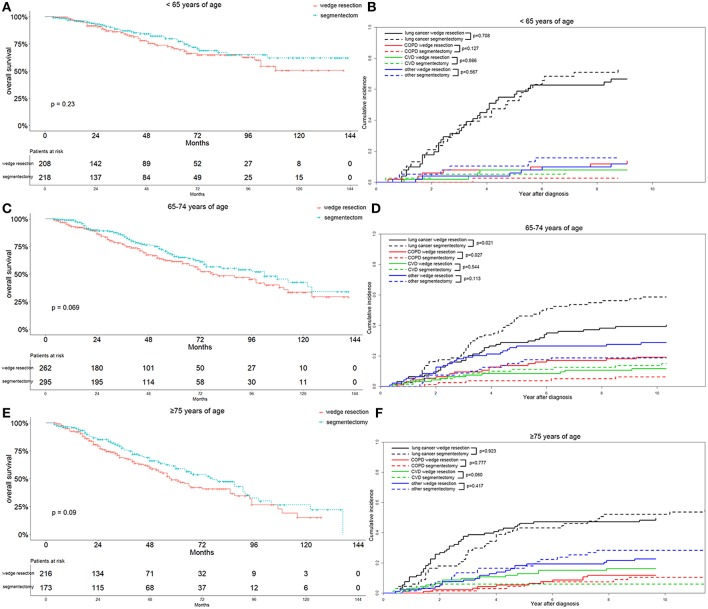
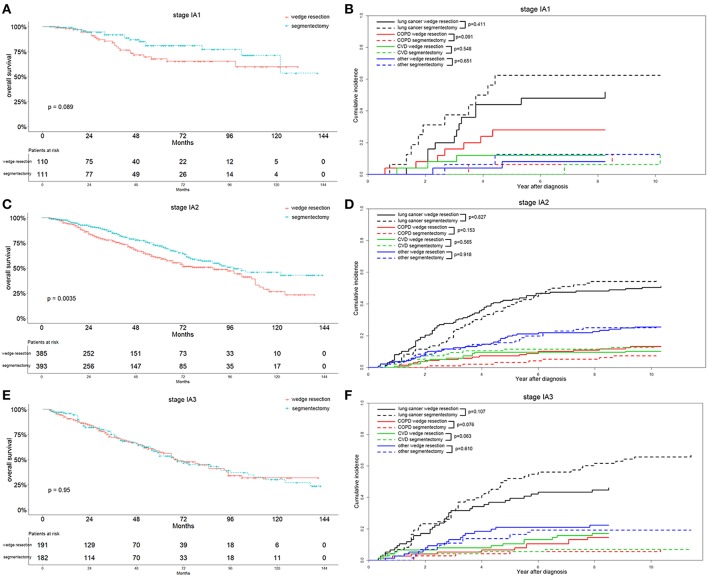
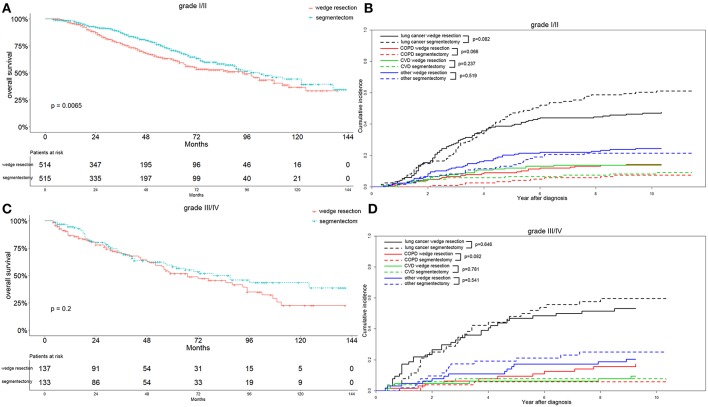
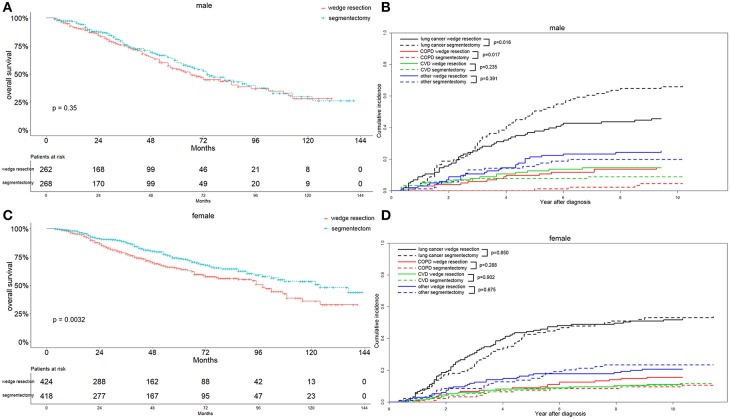
Limited resection has been carried out increasingly in early stage NSCLC as an alternative to standard lobectomy. This study aimed to investigate the differences in survival and long-term cause-specific mortality between wedge resection and segmentectomy for treatment of stage IA lung adenocarcinoma. Cases with primary lung adenocarcinoma that received wedge resection and segmentectomy between 2004 and 2015 were selected from the Surveillance, Epidemiology, and End Results (SEER) database. Propensity score matching was performed to balance the baseline covariates. Long-term cause-specific mortality was investigated through competing risk analysis. The overall survival (OS) was estimated with the Kaplan-Meier method with the log-rank test. Univariate and multivariate Cox proportional hazards regression analyses were performed to identify the independent prognostic factors. Of the 3,046 cases included, 2,360 and 686 cases underwent wedge resection and segmentectomy, respectively. After propensity score matching, 686 pairs were selected. Segmentectomy was associated with a significantly better OS in stage IA2, grade I/II, female, and married patients. The segmentectomy group had a higher lung-cancer specific mortality in 65-74 years of age, stage IA1 and IA3, male, and married patients, and a lower chronic obstructive pulmonary disease (COPD) specific mortality in ≤64 and 65-74 years of age, stage IA1, IA2, and IA3, all grade, male, and married patients. The cardiovascular disease (CVD) specific mortality was also lower in the segmentectomy group in ≥75 years of age, stage IA1 and IA3, and grade I/II patients. Wedge resection was inferior to segmentectomy in terms of OS regarding all included parameters. In most cases, the segmentectomy group had higher lung-cancer specific mortality and lower COPD and CVD specific mortality.
作为标准肺叶切除术的替代方法,早期非小细胞肺癌(NSCLC)的局限性切除术应用越来越多。本研究旨在探讨楔形切除术和肺段切除术治疗ⅠA期肺腺癌在生存率和长期特定病因死亡率方面的差异。从监测、流行病学和最终结果(SEER)数据库中选取2004年至2015年间接受楔形切除术和肺段切除术的原发性肺腺癌病例。进行倾向评分匹配以平衡基线协变量。通过竞争风险分析研究长期特定病因死亡率。采用Kaplan-Meier法和对数秩检验估计总生存期(OS)。进行单因素和多因素Cox比例风险回归分析以确定独立预后因素。纳入的3046例病例中,分别有2360例和686例接受了楔形切除术和肺段切除术。倾向评分匹配后,选取了686对。肺段切除术与ⅠA2期、Ⅰ/Ⅱ级、女性和已婚患者的OS显著更好相关。肺段切除术组在65 - 74岁、ⅠA1期和ⅠA3期、男性和已婚患者中肺癌特异性死亡率较高,在≤64岁和65 - 74岁、ⅠA1期、ⅠA2期和ⅠA3期、所有分级、男性和已婚患者中慢性阻塞性肺疾病(COPD)特异性死亡率较低。在≥75岁、ⅠA1期和ⅠA3期以及Ⅰ/Ⅱ级患者中,肺段切除术组的心血管疾病(CVD)特异性死亡率也较低。就所有纳入参数的OS而言,楔形切除术不如肺段切除术。在大多数情况下,肺段切除术组肺癌特异性死亡率较高,COPD和CVD特异性死亡率较低。