Shao Shengteng, Song Guisong, Wang Yuanyong, Yi Tengfei, Li Shuo, Chen Fuhui, Li Yang, Liu Xiaotong, Han Bin, Liu Yuhong
Department of Thoracic Surgery, The Affiliated Hospital of Qingdao University, Qingdao, China.
Front Oncol. 2022 Aug 23;12:946800. doi: 10.3389/fonc.2022.946800. eCollection 2022.
This study aimed to conduct a comparative analysis of the survival rates after segmentectomy, wedge resection, or lobectomy in patients with cStage IA lung squamous cell carcinoma (SCC).
We enrolled 4,316 patients who had cStage IA lung SCC from the Surveillance, Epidemiology, and End Results (SEER) database. The Cox proportional hazards model was conducted to recognize the potential risk factors for overall survival (OS) and lung cancer-specific survival (LCSS). To eliminate potential biases of included patients, the propensity score matching (PSM) method was used. OS and LCSS rates were compared among three groups stratified according to tumor size.
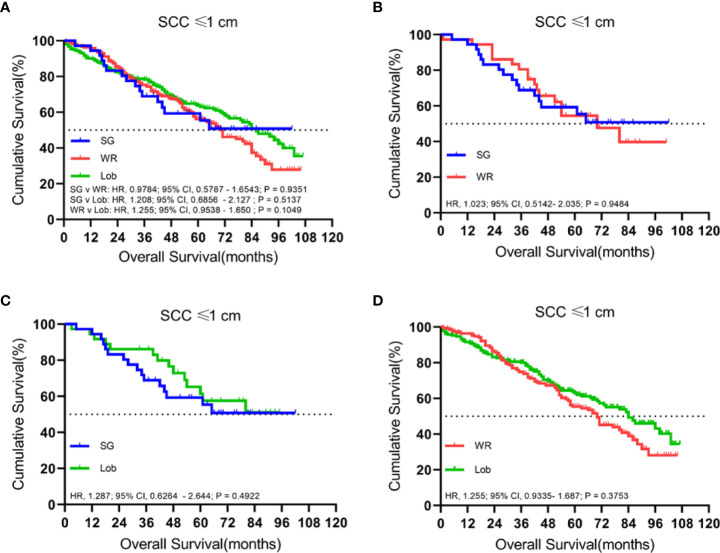
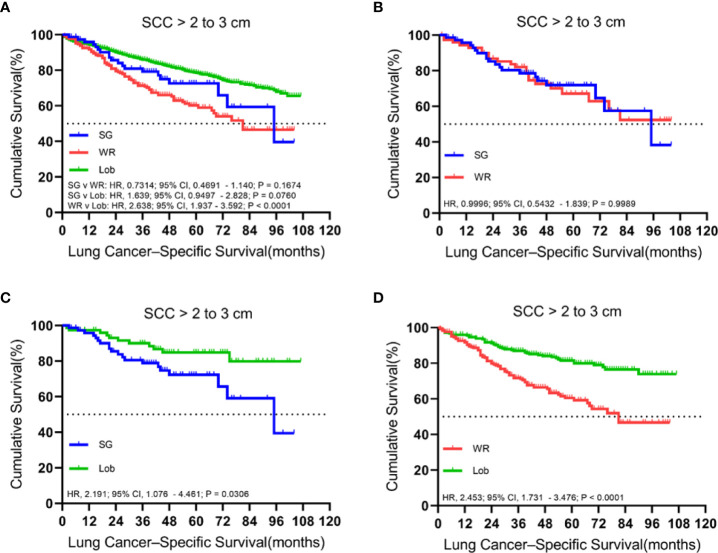
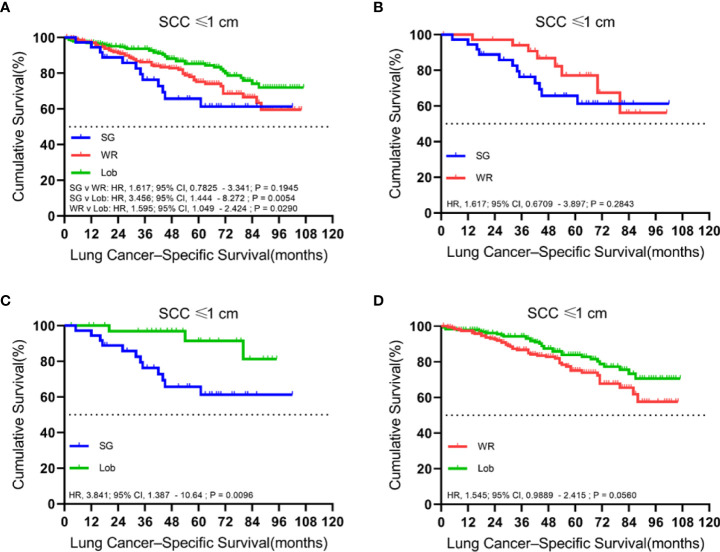
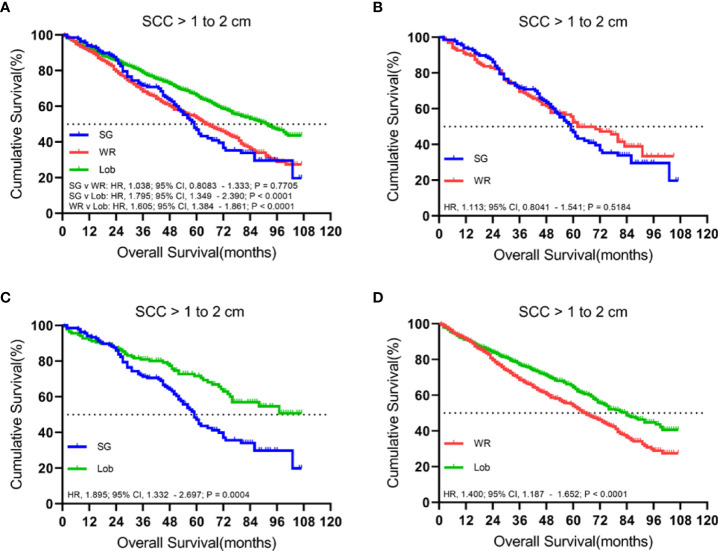
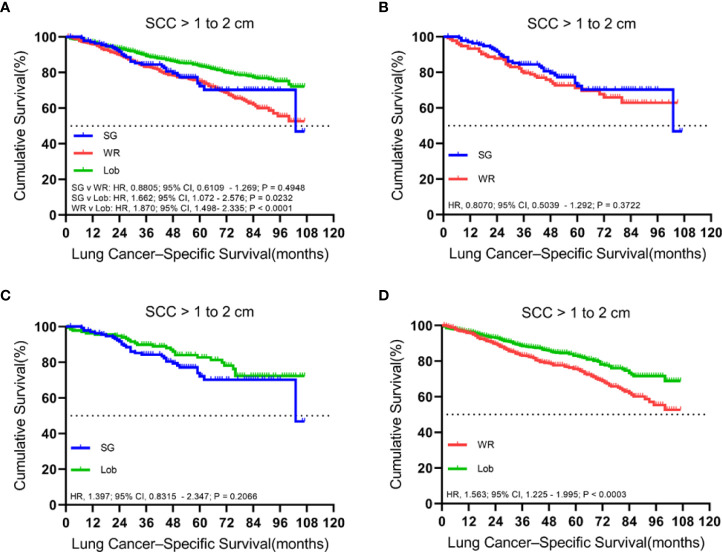
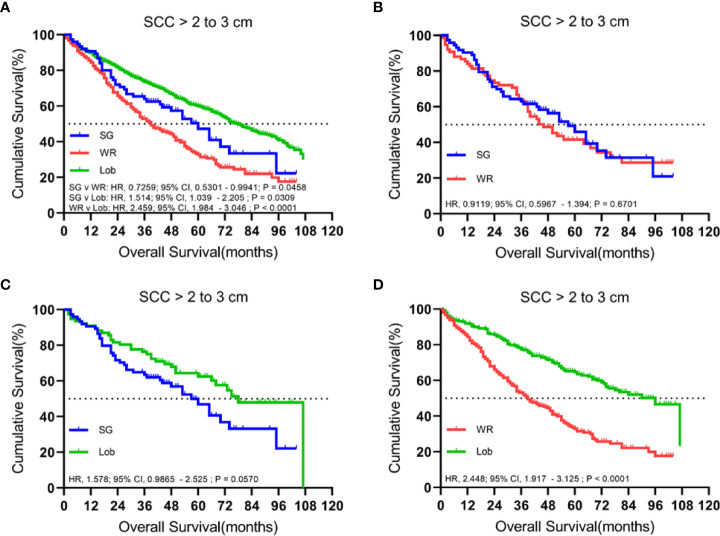
Kaplan-Meier analyses revealed no statistical differences in the rates of OS and LCSS between wedge resection (WR) and segmentectomy (SG) groups for patients who had cStage IA cancers. In patients with tumors ≤ 1 cm, LCSS favored lobectomy (Lob) compared to segmentectomy (SG), but a similar survival rate was obtained for wedge resection (WR) and lobectomy (Lob). For patients with tumors sized 1.1 to 2 cm, lobectomy had improved OS and LCSS rates compared to the segmentectomy or wedge resection groups, with the exception of a similar OS rate for lobectomy and segmentectomy. For tumors sized 2.1 to 3 cm, lobectomy had a higher rate of OS or LCSS than wedge resection or segmentectomy, except that lobectomy conferred a similar LCSS rate compared to segmentectomy. Multivariable analyses showed that patients aged ≥75 and tumor sizes of >2 to ≤3 cm were potential risk factors for OS and LCSS, while lobectomy and first malignant primary indicator were considered protective factors. The Cox proportional analysis also confirmed that male patients aged ≥65 to <75 were independent prognostic factors that are indicative of a worse OS rate.
The tumor size can influence the surgical procedure recommended for individuals with cStage IA lung SCC. For patients with tumors ≤1 cm, lobectomy is the recommended approach, and wedge resection or segmentectomy might be an alternative for those who cannot tolerate lobectomy if adequate surgical margin is achievable and enough nodes are sampled. For tumors >1 to ≤3 cm, lobectomy showed better survival outcomes than sublobar resection. Our findings require further validation by randomized controlled trial (RCT) or other evidence.
本研究旨在对cStage IA期肺鳞状细胞癌(SCC)患者行肺段切除术、楔形切除术或肺叶切除术后的生存率进行比较分析。
我们从监测、流行病学和最终结果(SEER)数据库中纳入了4316例cStage IA期肺SCC患者。采用Cox比例风险模型识别总生存(OS)和肺癌特异性生存(LCSS)的潜在危险因素。为消除纳入患者的潜在偏倚,使用了倾向评分匹配(PSM)方法。根据肿瘤大小将患者分为三组,比较三组的OS和LCSS率。
Kaplan-Meier分析显示,cStage IA期癌症患者的楔形切除术(WR)组和肺段切除术(SG)组之间的OS和LCSS率无统计学差异。对于肿瘤≤1 cm的患者,与肺段切除术(SG)相比,肺叶切除术(Lob)的LCSS更佳,但楔形切除术(WR)和肺叶切除术(Lob)的生存率相似。对于肿瘤大小为1.1至2 cm的患者,与肺段切除术或楔形切除术组相比,肺叶切除术的OS和LCSS率有所提高,但肺叶切除术和肺段切除术的OS率相似。对于肿瘤大小为2.1至3 cm的患者,肺叶切除术的OS或LCSS率高于楔形切除术或肺段切除术,但与肺段切除术相比,肺叶切除术的LCSS率相似。多变量分析显示,年龄≥75岁和肿瘤大小>2至≤3 cm的患者是OS和LCSS的潜在危险因素,而肺叶切除术和首个恶性原发性指标被视为保护因素。Cox比例分析还证实,年龄≥65至<75岁的男性患者是独立的预后因素,提示OS率较差。
肿瘤大小可影响cStage IA期肺SCC患者推荐的手术方式。对于肿瘤≤1 cm的患者,推荐行肺叶切除术,如果能获得足够的手术切缘并采集足够的淋巴结,对于无法耐受肺叶切除术的患者,楔形切除术或肺段切除术可能是一种替代方案。对于肿瘤>1至≤3 cm的患者,肺叶切除术的生存结果优于肺叶下切除术。我们的研究结果需要通过随机对照试验(RCT)或其他证据进行进一步验证。