Department of Medicine, Minneapolis Veterans Affairs Medical Center and University of Minnesota, Minneapolis, Minnesota, United States of America.
Division of Biostatistics, University of Minnesota, Minneapolis, Minnesota, United States of America.
PLoS One. 2019 Jul 23;14(7):e0219962. doi: 10.1371/journal.pone.0219962. eCollection 2019.
Chronic obstructive pulmonary disease (COPD) is an inflammatory lung disorder associated with lung microbiome dysbiosis. Although the upper airway microbiome is the source of the lung microbiome, the relationships between the oral, nasal, and sputum microbiota are incompletely understood. Our objective was to determine features that differentiate the oral, nasal, and sputum microbiome among subjects with stable COPD.
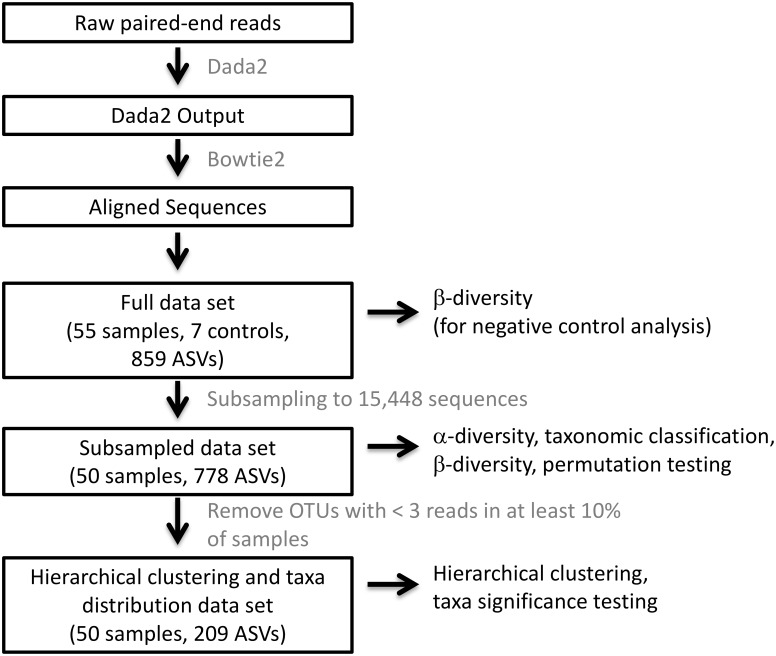
We recruited 15 current or former smokers to provide oral and sputum samples on day 1. On day 2, another oral sample and a nasal sample were obtained. Each sample and control underwent DNA extraction, 16S V4 rRNA amplification, 16S V4 sequencing, and qPCR of 16S rRNA. Data were analyzed using dada2 and R.
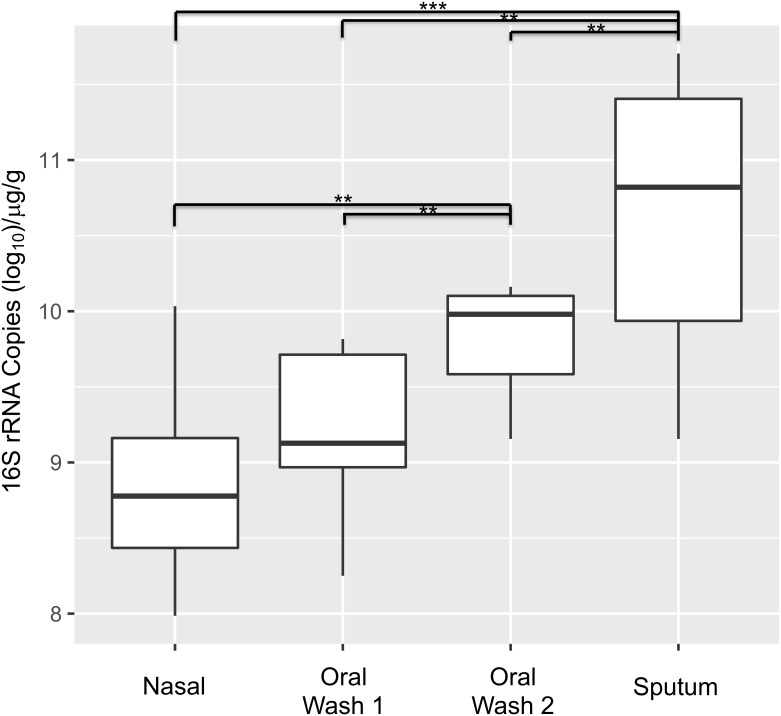
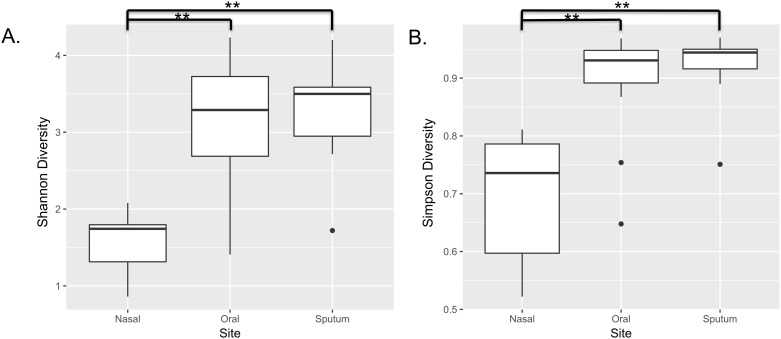
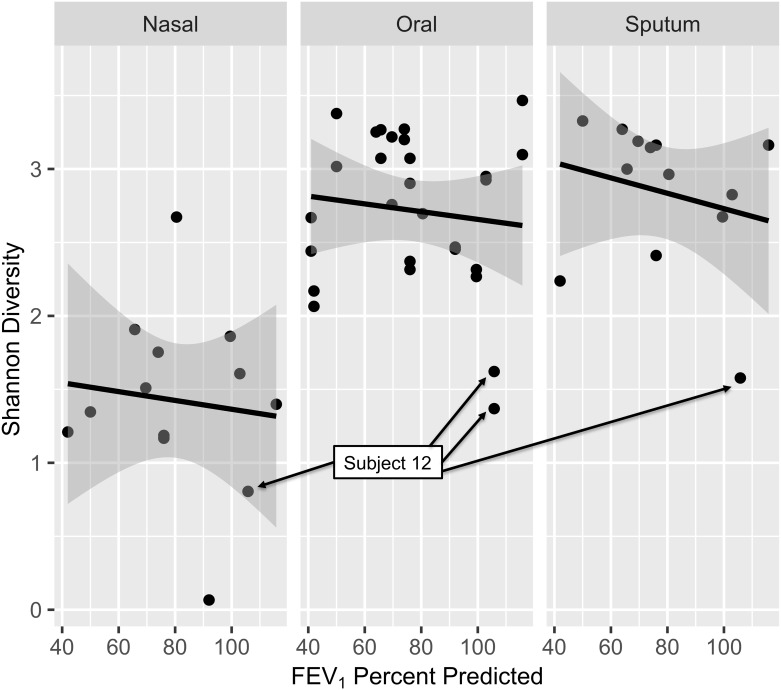
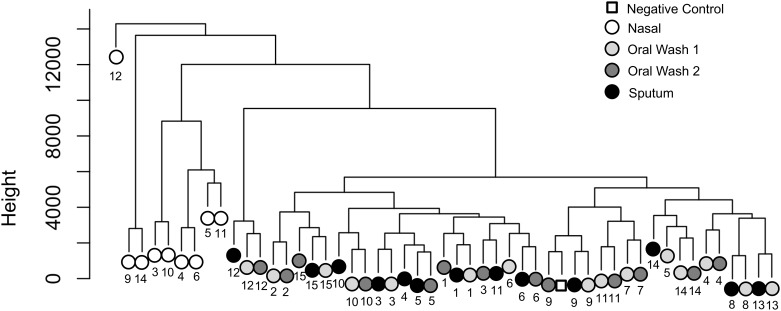
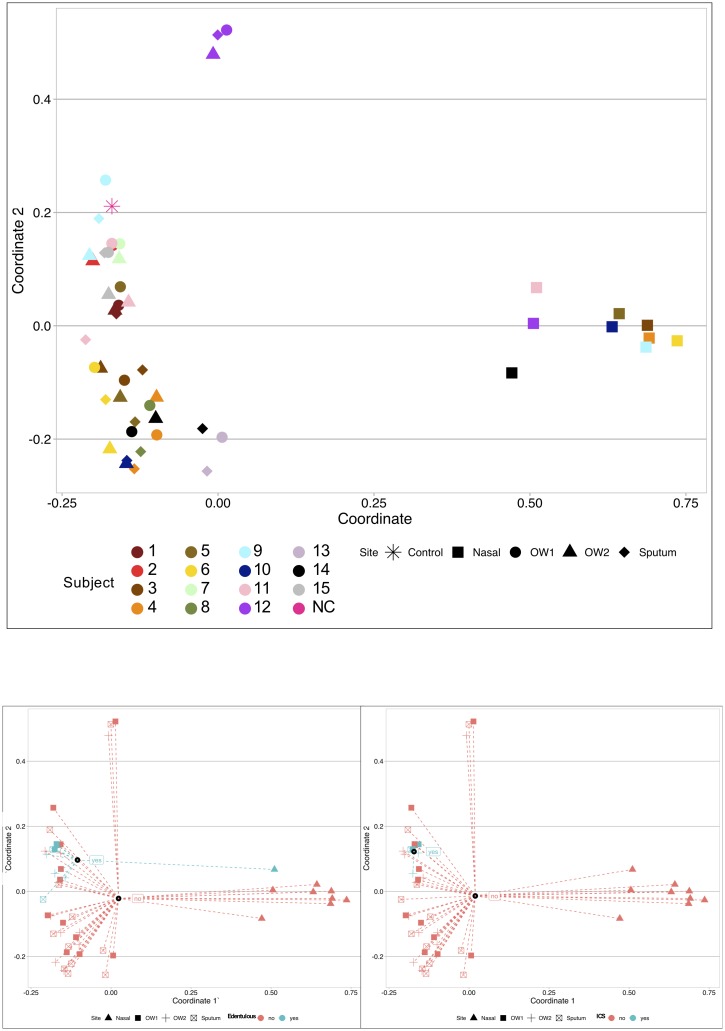
Most (14 of 15) subjects were male with a mean age of 65.2. One subject had no pulmonary obstruction, while 5 had mild COPD, 7 had moderate COPD, and 2 had severe COPD. Three subjects (20%) were current tobacco users and 2 subjects (13%) used inhaled corticosteroids (ICS). Subjects had a mean of 49.1 pack-years of tobacco exposure. Bacterial biomass was associated with anatomic site, but no differences in biomass were observed with age, FEV1 percent predicted (FEV1pp), ICS use, smoking status, or edentulous state. Shannon index was associated with site (lower nasal diversity than oral and sputum diversity, p<0.001), but not age, ICS use, FEV1pp, tobacco use, or edentulous state. β-diversity was illustrated by principal coordinate analysis using Bray-Curtis dissimilarity and PERMANOVA analyses, showing sample clustering by anatomic site (p = 0.001) with nasal samples forming a cluster separate from the combined oral wash samples and sputum samples. Clustering was also observed with ICS use (p = 0.029) and edentulous state (p = 0.019), while FEV1pp and current tobacco use were not significant. In an amplicon sequencing variant (ASV)-level analysis of oral samples using a linear regression model with Benjamini-Hochberg correction at an FDR<0.10, 10 ASVs were associated with age while no ASVs were associated with FEV1pp or smoking status. Sputum sample analysis demonstrated that 51 ASVs (25 unique genera) were associated with age, 61 ASVs (32 genera) were associated with FEV1pp, and no ASVs were associated with smoking status. In a combined dataset, the frequent exacerbator phenotype, rather than ICS use, was associated with decreased sputum Shannon diversity.
Among the upper airway microbiota of COPD subjects, anatomic site was associated with bacterial biomass, Shannon diversity, and β-diversity. ICS use and edentulous state were both associated with β-diversity. Age was associated with taxa relative abundance in oral and sputum samples, while FEV1pp was associated with taxa relative abundance in sputum samples only.
慢性阻塞性肺疾病(COPD)是一种与肺部微生物组失调相关的肺部炎症性疾病。尽管上呼吸道微生物组是肺部微生物组的来源,但口腔、鼻腔和痰液微生物组之间的关系尚不完全清楚。我们的目的是确定区分稳定期 COPD 患者口腔、鼻腔和痰液微生物组的特征。
我们招募了 15 名现吸烟者或前吸烟者,让他们在第 1 天提供口腔和痰液样本。第 2 天,采集另一份口腔样本和鼻腔样本。每个样本和对照样本均进行 DNA 提取、16S V4 rRNA 扩增、16S V4 测序和 16S rRNA 的 qPCR。使用 dada2 和 R 进行数据分析。
大多数(15 名中的 14 名)受试者为男性,平均年龄为 65.2 岁。1 名受试者没有肺部阻塞,5 名受试者患有轻度 COPD,7 名患有中度 COPD,2 名患有重度 COPD。3 名受试者(20%)为现吸烟,2 名受试者(13%)使用吸入皮质激素(ICS)。受试者平均有 49.1 包年的烟草暴露量。细菌生物量与解剖部位有关,但与年龄、FEV1 占预计值百分比(FEV1pp)、ICS 使用、吸烟状况或无牙状态无关。香农指数与部位有关(鼻腔多样性低于口腔和痰液多样性,p<0.001),但与年龄、ICS 使用、FEV1pp、吸烟状况或无牙状态无关。主坐标分析(使用 Bray-Curtis 不相似性和 PERMANOVA 分析)显示了基于β多样性的样本聚类,表明样本聚类与解剖部位有关(p = 0.001),鼻腔样本与口腔冲洗样本和痰液样本聚类分离。ICS 使用(p = 0.029)和无牙状态(p = 0.019)也观察到聚类,而 FEV1pp 和现吸烟状况则不显著。在口腔样本的扩增子测序变体(ASV)水平分析中,使用 FDR<0.10 的 Benjamini-Hochberg 校正的线性回归模型,有 10 个 ASV 与年龄有关,而没有 ASV 与 FEV1pp 或吸烟状况有关。痰液样本分析表明,51 个 ASV(25 个独特属)与年龄有关,61 个 ASV(32 个属)与 FEV1pp 有关,没有 ASV 与吸烟状况有关。在一个综合数据集,频繁急性加重表型,而不是 ICS 使用,与痰液 Shannon 多样性降低有关。
在 COPD 患者的上呼吸道微生物群中,解剖部位与细菌生物量、Shannon 多样性和β多样性有关。ICS 使用和无牙状态均与β多样性有关。年龄与口腔和痰液样本中的分类群相对丰度有关,而 FEV1pp 仅与痰液样本中的分类群相对丰度有关。