Department of Anesthesiology, Michigan Medicine, University of Michigan, Ann Arbor.
Department of Emergency Medicine, Michigan Medicine, University of Michigan, Ann Arbor.
JAMA Netw Open. 2019 Jul 3;2(7):e197584. doi: 10.1001/jamanetworkopen.2019.7584.
Increased patient acuity, decreased intensive care unit (ICU) bed availability, and a shortage of intensivist physicians have led to strained ICU capacity. The resulting increase in emergency department (ED) boarding time for patients requiring ICU-level care has been associated with worse outcomes.
To determine the association of a novel ED-based ICU, the Emergency Critical Care Center (EC3), with 30-day mortality and inpatient ICU admission.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used electronic health records of all ED visits between September 1, 2012, and July 31, 2017, with a documented clinician encounter at a large academic medical center in the United States with approximately 75 000 adult ED visits per year. The pre-EC3 cohort included ED patients from September 2, 2012, to February 15, 2015, when the EC3 opened, and the post-EC3 cohort included ED patients from February 16, 2015, to July 31, 2017. Data analyses were conducted from March 2, 2018, to May 28, 2019.
Implementation of EC3, an ED-based ICU designed to provide rapid initiation of ICU-level care in the ED setting and seamless transition to inpatient ICUs.
The main outcomes were 30-day mortality among ED patients and rate of ED to ICU admission.
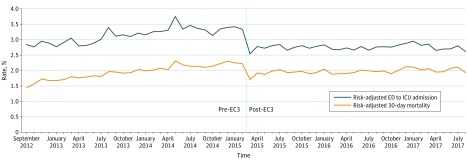
A total of 349 310 visits from a consecutive sample of ED patients (mean [SD] age, 48.5 [19.7] years; 189 709 [54.3%] women) were examined; the pre-EC3 cohort included 168 877 visits and the post-EC3 cohort included 180 433 visits. Implementation of EC3 was associated with a statistically significant reduction in risk-adjusted 30-day mortality among all ED patients (pre-EC3, 2.13%; post-EC3, 1.83%; adjusted odds ratio, 0.85; 95% CI, 0.80-0.90; number needed to treat, 333 patient encounters; 95% CI, 256-476). The risk-adjusted rate of ED admission to ICU decreased with implementation of EC3 (pre-EC3, 3.2%; post-EC3, 2.7%; adjusted odds ratio, 0.80; 95% CI, 0.76-0.83; number needed to treat, 179 patient encounters; 95% CI, 149-217).
Implementation of a novel ED-based ICU was associated with improved 30-day survival and reduced inpatient ICU admission. Additional research is warranted to further explore the value of this novel care delivery model in various health care systems.
患者病情加重、重症监护病房(ICU)床位减少以及重症医师短缺,导致 ICU 容量紧张。由此导致需要 ICU 级护理的患者在急诊科(ED)滞留时间增加,与预后较差有关。
确定新型 ED 基础 ICU,即紧急关键护理中心(EC3)与 30 天死亡率和住院 ICU 入院率的相关性。
设计、地点和参与者:这是一项回顾性队列研究,使用了美国一家大型学术医疗中心 2012 年 9 月 1 日至 2017 年 7 月 31 日期间所有 ED 就诊的电子健康记录,这些患者在该中心就诊时有临床医生记录。该研究的预 EC3 队列包括 2012 年 9 月 2 日至 2015 年 2 月 15 日期间就诊的 ED 患者,EC3 于 2015 年 2 月 16 日至 2017 年 7 月 31 日期间就诊的 ED 患者被归入后 EC3 队列。数据分析于 2018 年 3 月 2 日至 2019 年 5 月 28 日进行。
EC3 的实施,这是一种 ED 基础 ICU,旨在在 ED 环境中快速启动 ICU 级护理,并与住院 ICU 顺利过渡。
主要结局为 ED 患者 30 天死亡率和 ED 至 ICU 入院率。
共检查了连续抽样的 ED 患者的 349310 次就诊(平均[SD]年龄,48.5[19.7]岁;189709[54.3%]为女性);预 EC3 队列包括 168877 次就诊,后 EC3 队列包括 180433 次就诊。EC3 的实施与所有 ED 患者的风险调整后 30 天死亡率显著降低相关(预 EC3 组为 2.13%;后 EC3 组为 1.83%;调整后的优势比,0.85;95%CI,0.80-0.90;需要治疗的人数,333 例患者;95%CI,256-476)。EC3 实施后,ED 至 ICU 入院率的风险调整也降低(预 EC3 组为 3.2%;后 EC3 组为 2.7%;调整后的优势比,0.80;95%CI,0.76-0.83;需要治疗的人数,179 例患者;95%CI,149-217)。
新型 ED 基础 ICU 的实施与 30 天生存率的提高和住院 ICU 入院率的降低相关。需要进一步研究以进一步探索这种新型护理模式在各种医疗保健系统中的价值。