Urso Felice, Catalano Daniele, Petrovic Ileana Suprina, Boero Enrico, Berchialla Paola, Vetrugno Luigi, Silengo Daniela
Anesthesia and Intensive Care Unit, Ospedale San Giovanni Bosco, Turin, Italy.
Department of Clinical and Biological Sciences, University of Turin, Turin, Italy.
J Anesth Analg Crit Care. 2025 Jul 10;5(1):42. doi: 10.1186/s44158-025-00262-x.
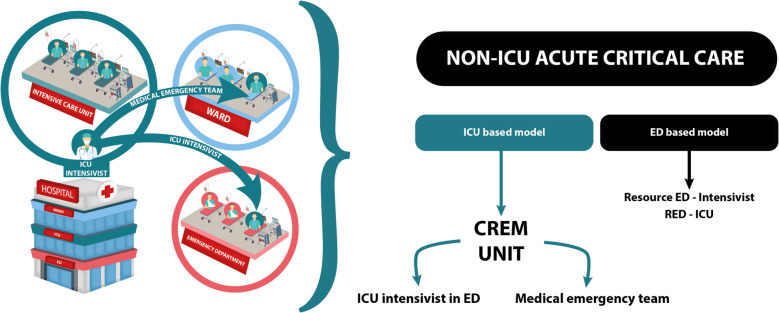
Boarding of critically ill patients in the emergency department (ED) is an emerging problem that increases mortality. We have developed a "CREM Unit (critical emergency medicine unit)" led by an anesthetist-intensivist who manages critical patients directly in the ED. This study aims to assess whether the CREM Unit is an effective model for mitigating the boarding of critical patients in the ED and the impact of this on mortality.
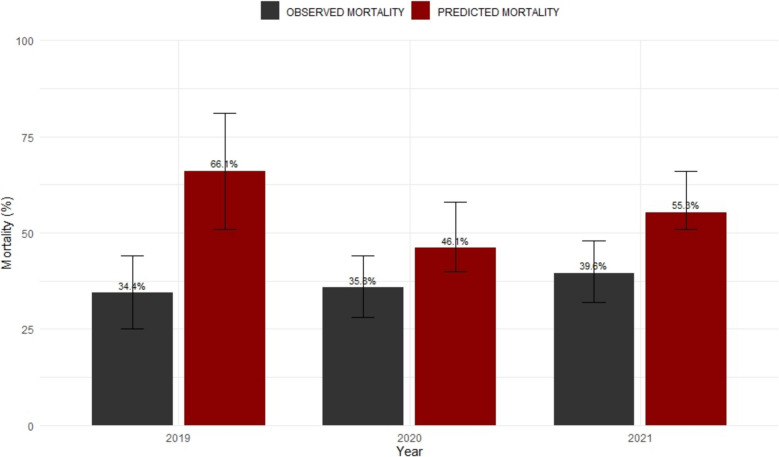
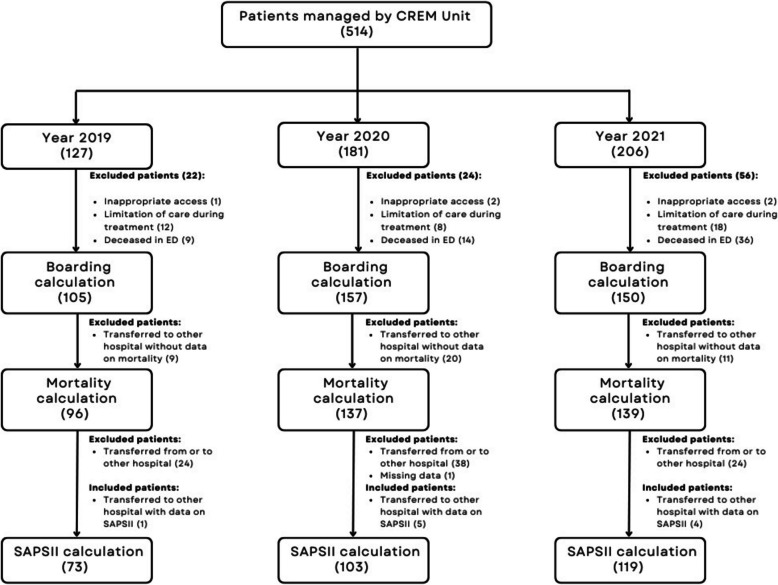
This is a retrospective observational study. We collected all patients assigned to the CREM Unit from January 1, 2019, to December 31, 2021. As our primary endpoints, we calculated ED boarding rate and the impact of boarding time on mortality. As a secondary endpoint, we compared observed 28-day mortality to Simplified Acute Physiology Score (SAPS II) predicted mortality.
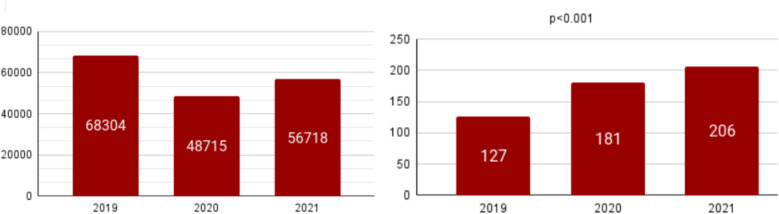
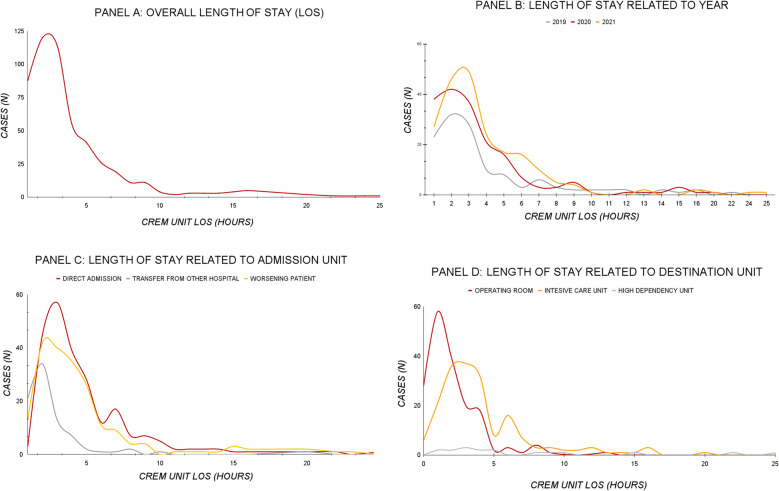
Patients managed by the CREM unit were 127 in 2019, 181 in 2020, and 206 in 2021, with a clear upward trend, for a total of 514 patients (p < 0.001). Overall boarding rate was 13.9%, and length of stay in ED was not associated with an increased mortality (p = 0.399). Observed mortality was compared with expected mortality, estimated from the SAPS II score for a group of inpatients (n = 295). Moreover, the median value of SAPS II for inpatients was 54 (40.5-69.0), with an expected mortality of 55.3%, while the observed mortality was 36.8% (95% CI 31.9% to 42.1%, p < 0.0001).
Over the years, the number of patients assigned to the CREM Unit has grown steadily. These data suggest that the CREM Unit cares for a significant number of critically ill patients and could have a well-defined role both in keeping their boarding low and may contribute to reducing its impact on mortality.
急诊科(ED)收治危重症患者是一个新出现的问题,会增加死亡率。我们设立了一个由麻醉科重症医学专家领导的“CREM单元(危重症急救医学单元)”,该专家在急诊科直接管理危重症患者。本研究旨在评估CREM单元是否是减轻急诊科危重症患者收治压力的有效模式,以及这对死亡率的影响。
这是一项回顾性观察研究。我们收集了2019年1月1日至2021年12月31日期间分配到CREM单元的所有患者。作为主要终点,我们计算了急诊科收治率以及收治时间对死亡率的影响。作为次要终点,我们将观察到的28天死亡率与简化急性生理学评分(SAPS II)预测的死亡率进行了比较。
2019年由CREM单元管理的患者有127例,2020年有181例,2021年有206例,呈明显上升趋势,共计514例患者(p<0.001)。总体收治率为13.9%,在急诊科的住院时间与死亡率增加无关(p = 0.399)。将观察到的死亡率与根据一组住院患者(n = 295)的SAPS II评分估计的预期死亡率进行了比较。此外,住院患者SAPS II的中位数为54(40.5 - 69.0),预期死亡率为55.3%,而观察到的死亡率为36.8%(95%CI 31.9%至42.1%,p<0.0001)。
多年来,分配到CREM单元的患者数量稳步增长。这些数据表明,CREM单元照料了大量危重症患者,在保持低收治率方面可能具有明确作用,并且可能有助于降低其对死亡率的影响。