Harbor-UCLA Medical Center, Torrance, California, United States of America.
Emergency and Trauma Centre, The Alfred, Melbourne, Australia.
PLoS One. 2019 Jul 24;14(7):e0220179. doi: 10.1371/journal.pone.0220179. eCollection 2019.
Injury accounts for more than 5.8 million deaths globally with an increasing burden in the developing world. In Kenya, trauma is one of the top 10 leading causes of death. However, no formal continuous injury surveillance systems are in place to inform injury prevention, pre-hospital care or emergency department management. The aim of this study was to implement a hospital-based trauma registry to characterize high acuity injuries presenting to a private tertiary, teaching and referral hospital in Kenya.
From January to December 2015, data was prospectively collected at a private tertiary, teaching and referral hospital in Nairobi, Kenya. Patients presenting with a traumatic injury for the first time who were admitted to the hospital for at least 48 hours were included in the study. Basic information pertaining to demographics, details of the injury, pre-hospital care and transport, hospital-based management, length of stay and disposition were collected. An injury severity score (ISS) was calculated on each patient and stratified by the mechanism of injury. Descriptive statistics and multivariate logistic regression were used to analyze data and assess risk factors associated with injury severity.
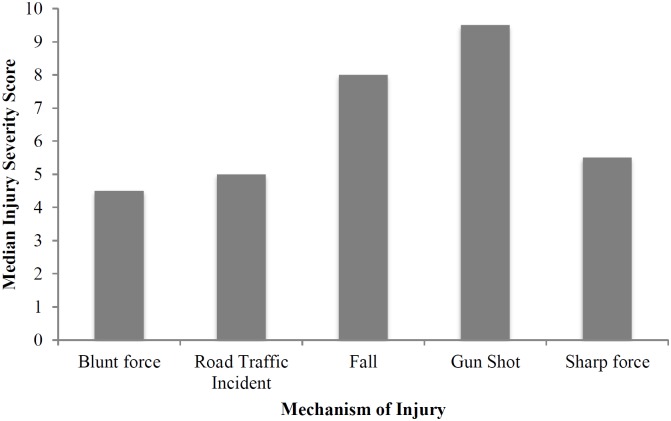
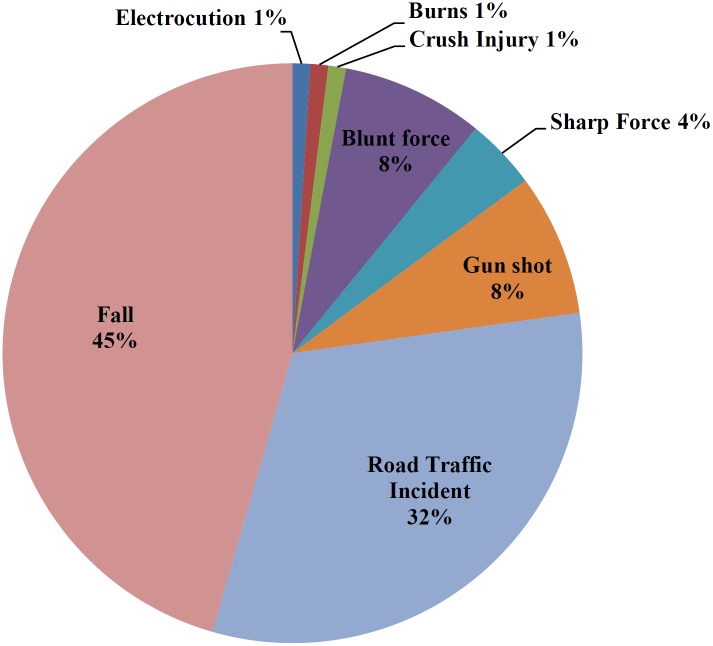
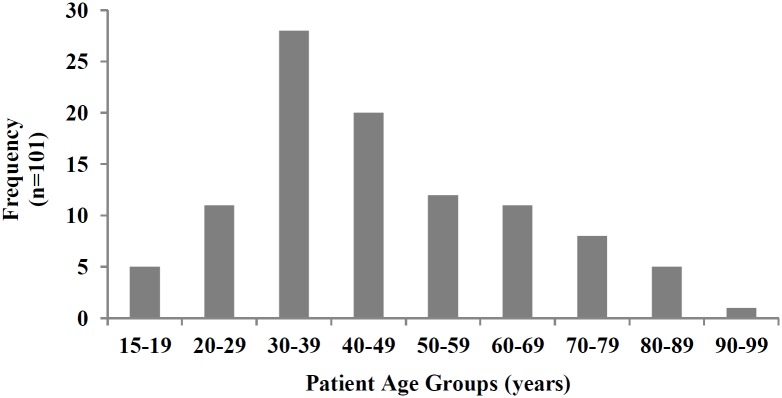
There were 101 patients included in the study, the majority of whom were 30 to 39 years of age and male (63%). Seventy-one per cent of patients had a preexisting medical condition with hypertension (26%) and diabetes (13%) being the most common. The most common mechanism of injury was fall (46%) followed by road traffic incidents (RTI) (32%). Most injuries took place at home (43%). Most RTI were caused by cars (63%), with the driver being the most frequently injured (38%). The most common mode of arrival to the emergency department was by private car (72%). The median time between the accident and arrival at the emergency department was 1hr 10 minutes. The majority of the patients had injuries to one area (83%) with the extremities/bony pelvis (72%) being the most common. The median Injury Severity Score was 5 (range 1-34) with the majority (90%) classified as minor injuries (ISS<12). The highest severity of injury as determined by ISS was seen in gunshot wounds.
Injured patients in Kenya showed concordance with prior studies looking at injury prevalence in the developing world when looking at demographics and place of injury. However, differences were found when looking at the mechanism of injury, with falls surpassing road traffic incidents. A delayed presentation to the hospital was also noted in this patient population. Given the rate of traumatic injuries in Kenya and their contribution to morbidity, mortality and overall healthcare costs, there is a need to implement formal trauma registries in all major hospitals in Kenya to generate more data that can be used to improve injury prevention, the overall trauma system and enhance training and preparedness.
全球范围内,伤害导致的死亡人数超过 580 万,且在发展中国家这一负担呈上升趋势。在肯尼亚,创伤是导致死亡的十大原因之一。然而,目前没有正式的连续伤害监测系统来为伤害预防、院前护理或急诊科管理提供信息。本研究旨在建立一个基于医院的创伤登记系统,以描述在肯尼亚的一家私立三级教学和转诊医院就诊的高 acuity 创伤患者。
2015 年 1 月至 12 月,在肯尼亚内罗毕的一家私立三级教学和转诊医院进行前瞻性数据收集。研究纳入首次因创伤性损伤而首次就诊并在医院至少住院 48 小时的患者。收集与人口统计学、损伤细节、院前护理和转运、医院管理、住院时间和处置相关的基本信息。对每位患者计算损伤严重程度评分(ISS),并按损伤机制进行分层。使用描述性统计和多变量逻辑回归分析数据,并评估与损伤严重程度相关的危险因素。
本研究共纳入 101 例患者,其中大多数为 30 至 39 岁,男性(63%)。71%的患者有既往病史,其中高血压(26%)和糖尿病(13%)最为常见。最常见的损伤机制是跌倒(46%),其次是道路交通伤害(RTI)(32%)。大多数损伤发生在家庭(43%)。大多数 RTI 是由汽车引起的(63%),驾驶员是最常受伤的(38%)。最常见的到达急诊科的方式是私家车(72%)。事故发生与到达急诊科之间的中位时间为 1 小时 10 分钟。大多数患者只有一处损伤(83%),最常见的是四肢/骨盆(72%)。损伤严重程度评分中位数为 5(范围 1-34),其中大多数(90%)被归类为轻伤(ISS<12)。ISS 最高的严重程度损伤见于枪伤。
肯尼亚的受伤患者在人口统计学和受伤地点方面与之前研究中发展中国家的损伤流行情况一致。然而,在损伤机制方面存在差异,跌倒超过道路交通伤害。本患者人群还存在就诊时间延迟的情况。鉴于肯尼亚创伤发生率及其对发病率、死亡率和整体医疗保健费用的影响,有必要在肯尼亚所有主要医院实施正式的创伤登记系统,以生成更多数据,用于改善伤害预防、整体创伤系统,并加强培训和准备工作。