Neuroscience Research Australia, 139 Barker Street, Randwick, NSW, 2031, Australia.
School of Medical Sciences, University of New South Wales, Kensington, NSW, 2052, Australia.
Crit Care. 2019 Jul 24;23(1):261. doi: 10.1186/s13054-019-2544-0.
For every day a person is dependent on mechanical ventilation, respiratory and cardiac complications increase, quality of life decreases and costs increase by > $USD 1500. Interventions that improve respiratory muscle function during mechanical ventilation can reduce ventilation duration. The aim of this pilot study was to assess the feasibility of employing an abdominal functional electrical stimulation (abdominal FES) training program with critically ill mechanically ventilated patients. We also investigated the effect of abdominal FES on respiratory muscle atrophy, mechanical ventilation duration and intensive care unit (ICU) length of stay.
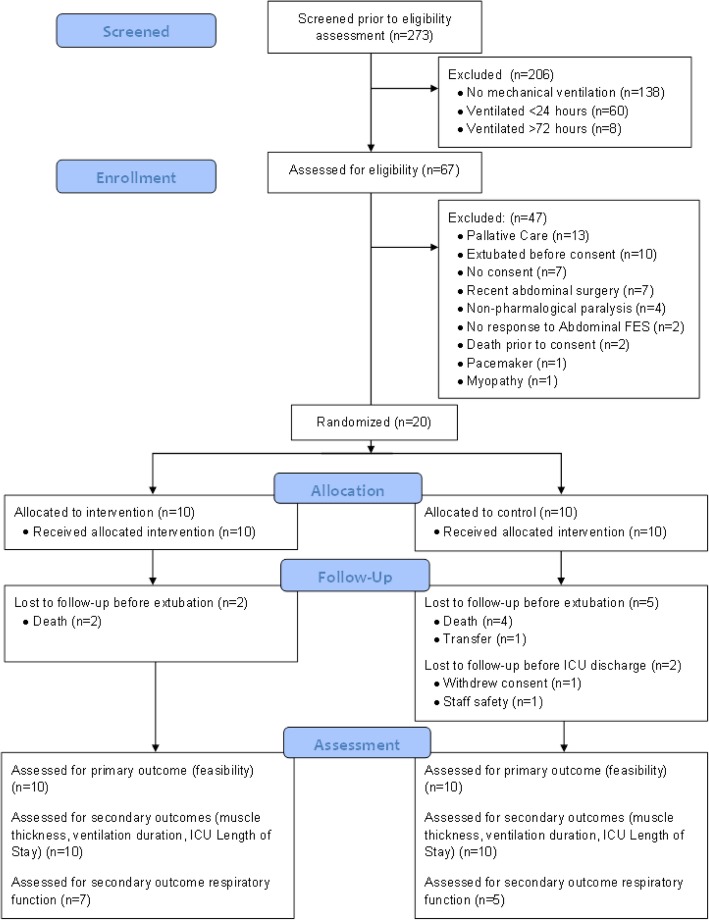
Twenty critically ill mechanically ventilated participants were recruited over a 6-month period from one metropolitan teaching hospital. They were randomly assigned to receive active or sham (control) abdominal FES for 30 min, twice per day, 5 days per week, until ICU discharge. Feasibility was assessed through participant compliance to stimulation sessions. Abdominal and diaphragm muscle thickness were measured using ultrasound 3 times in the first week, and weekly thereafter by a blinded assessor. Respiratory function was recorded when the participant could first breathe independently and at ICU discharge, with ventilation duration and ICU length of stay also recorded at ICU discharge by a blinded assessor.
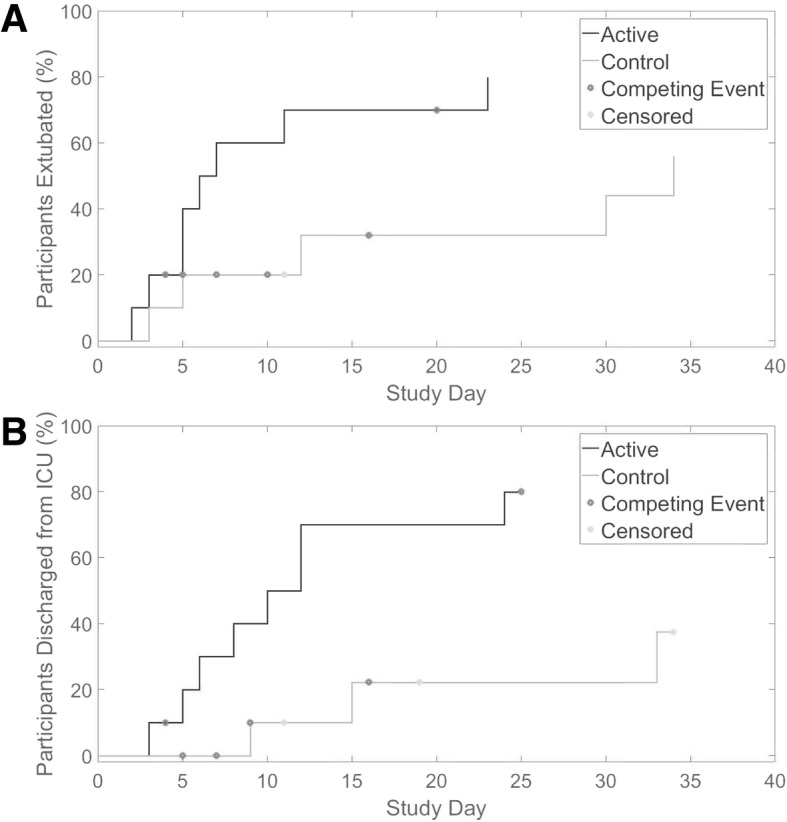
Fourteen of 20 participants survived to ICU discharge (8, intervention; 6, control). One control was transferred before extubation, while one withdrew consent and one was withdrawn for staff safety after extubation. Median compliance to stimulation sessions was 92.1% (IQR 5.77%) in the intervention group, and 97.2% (IQR 7.40%) in the control group (p = 0.384). While this pilot study is not adequately powered to make an accurate statistical conclusion, there appeared to be no between-group thickness changes of the rectus abdominis (p = 0.099 at day 3), diaphragm (p = 0.652 at day 3) or combined lateral abdominal muscles (p = 0.074 at day 3). However, ICU length of stay (p = 0.011) and ventilation duration (p = 0.039) appeared to be shorter in the intervention compared to the control group.
Our compliance rates demonstrate the feasibility of using abdominal FES with critically ill mechanically ventilated patients. While abdominal FES did not lead to differences in abdominal muscle or diaphragm thickness, it may be an effective method to reduce ventilation duration and ICU length of stay in this patient group. A fully powered study into this effect is warranted.
The Australian New Zealand Clinical Trials Registry, ACTRN12617001180303. Registered 9 August 2017.
患者依赖机械通气的天数每增加一天,呼吸和心脏并发症的发生率就会增加,生活质量下降,费用增加超过 1500 美元。在机械通气期间改善呼吸肌功能的干预措施可以减少通气时间。本研究旨在评估对机械通气的危重症患者进行腹部功能性电刺激(abdominal FES)训练方案的可行性。我们还研究了腹部 FES 对呼吸肌萎缩、机械通气时间和重症监护病房(ICU)住院时间的影响。
在为期 6 个月的时间里,我们从一家大都市教学医院招募了 20 名接受机械通气的危重症患者。他们被随机分配接受主动或假(对照)腹部 FES,每天两次,每次 30 分钟,每周 5 天,直到 ICU 出院。通过患者对刺激治疗的依从性来评估可行性。在第一周内,由一位盲法评估者使用超声测量腹部和膈肌厚度 3 次,此后每周测量一次。当患者可以首次自主呼吸时和 ICU 出院时,记录呼吸功能,并由一位盲法评估者记录通气时间和 ICU 住院时间。
20 名参与者中有 14 名存活至 ICU 出院(8 名,干预组;6 名,对照组)。1 名对照组在拔管前转院,1 名对照组在拔管前撤回同意,1 名对照组在拔管后因员工安全问题撤回。干预组刺激治疗的中位依从率为 92.1%(IQR 5.77%),对照组为 97.2%(IQR 7.40%)(p=0.384)。虽然本研究的样本量不足以进行准确的统计学结论,但两组间腹直肌(第 3 天,p=0.099)、膈肌(第 3 天,p=0.652)或外侧腹肌(第 3 天,p=0.074)的厚度均无明显变化。然而,与对照组相比,干预组的 ICU 住院时间(p=0.011)和通气时间(p=0.039)似乎更短。
我们的依从率表明,使用腹部 FES 对机械通气的危重症患者是可行的。尽管腹部 FES 并没有导致腹部肌肉或膈肌厚度的差异,但它可能是减少该患者群体通气时间和 ICU 住院时间的有效方法。有必要进行一项充分的研究来验证这种效果。
澳大利亚和新西兰临床试验注册中心,ACTRN12617001180303。2017 年 8 月 9 日注册。