Clinic of Cardiology, Bursa Yüksek İhtisas Training and Research Hospital, Bursa, Turkey
Clinic of Cardiology, Ankara Atatürk Training and Research Hospital, Ankara, Turkey
Balkan Med J. 2019 Oct 28;36(6):324-330. doi: 10.4274/balkanmedj.galenos.2019.2019.4.88. Epub 2019 Jul 26.
Idiopathic premature ventricular contractions are frequently detected ventricular arrhythmias, and radiofrequency ablation is an effectively treatment for improving symptoms and eliminating premature ventricular contractions. Studies have reported a relationship between an elevated epicardial adipose tissue thickness and myocardial structural pathologies. However, the association between epicardial adipose tissue thickness and success rates of premature ventricular contraction ablation has not yet been investigated.
To assess the relationship between epicardial adipose tissue thickness and success rates of premature ventricular contraction ablation.
Retrospective case-control study.
This study enrolled a total of 106 consecutive patients who have had a high premature ventricular contraction burden of >10,000/24-h assessed using ambulatory Holter monitorization and underwent catheter ablation. A frequency of premature ventricular contractions of more than 10,000/day was defined as frequent premature ventricular contraction. Epicardial adipose tissue thickness was measured using 2D transthoracic echocardiography. A successful ablation was defined as >80% decrease in pre-procedural premature ventricular contraction attacks with the same morphology during 24-h Holter monitorization after a 1-month follow-up visit from an ablation procedure.
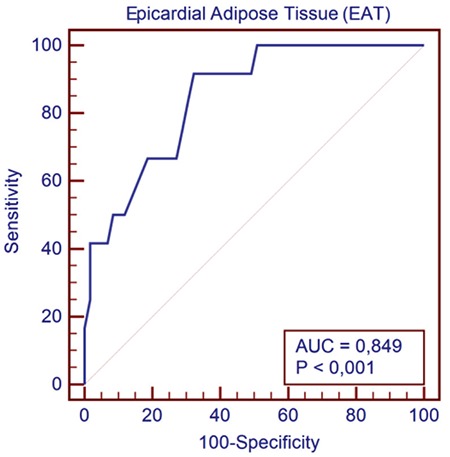
Successful premature ventricular contraction ablation was achieved in 87 (82.1%) patients. Epicardial adipose tissue thickness was significantly higher in patients with unsuccessful ablation (p<0.001). Procedure time, total fluoroscopy time, and radiofrequency ablation time were statistically higher in the unsuccessful group (p<0.001). Stepwise multivariate logistic regression analysis showed that epicardial adipose tissue thickness and pseudo-delta wave time were independently associated with procedural success (both p values <0.001). In the receiver-operating curve analysis, epicardial adipose tissue thickness was found to be an important predictor for procedural success (area under the receiver-operating characteristic curve= 0.85, p=0.001), with a cutoff value of 7.7 mm, a sensitivity of 92%, and a specificity of 68%.
Epicardial adipose tissue thickness is higher in patients with premature ventricular contraction ablation failure, which may be indicative of procedural success.
特发性室性早搏是常见的室性心律失常,射频消融是改善症状和消除室性早搏的有效治疗方法。研究报道心外膜脂肪组织厚度与心肌结构病变之间存在相关性。然而,心外膜脂肪组织厚度与室性早搏消融成功率之间的关系尚未得到研究。
评估心外膜脂肪组织厚度与室性早搏消融成功率之间的关系。
回顾性病例对照研究。
本研究共纳入 106 例连续患者,这些患者通过动态 Holter 监测评估室性早搏负荷>10000/24 h,接受导管消融治疗。每日室性早搏>10000 次定义为频发室性早搏。使用二维经胸超声心动图测量心外膜脂肪组织厚度。消融成功定义为消融后 1 个月随访期间 24 h Holter 监测到相同形态的室性早搏减少>80%。
87 例(82.1%)患者成功进行了室性早搏消融。消融不成功组患者的心外膜脂肪组织厚度明显较高(p<0.001)。不成功组的手术时间、总透视时间和射频消融时间均显著较高(p<0.001)。逐步多变量逻辑回归分析显示,心外膜脂肪组织厚度和假性δ波时间与手术成功率独立相关(p 值均<0.001)。在受试者工作特征曲线分析中,心外膜脂肪组织厚度是手术成功率的重要预测指标(曲线下面积为 0.85,p=0.001),截断值为 7.7mm,灵敏度为 92%,特异性为 68%。
消融失败的室性早搏患者心外膜脂肪组织厚度较高,可能提示手术成功率。