Gabaldo Krešimir, Sutlić Željko, Mišković Domagoj, Knežević Praveček Marijana, Prvulović Đeiti, Vujeva Božo, Cvitkušić Lukenda Katica, Hadžibegović Irzal
1Cardiology Department, Dr. Josip Benčević General Hospital, Slavonski Brod, Croatia; 2Department of Cardiac Surgery, Dubrava University Hospital, Zagreb, Croatia; 3Faculty of Medicine, Josip Juraj Strossmayer University of Osijek, Osijek, Croatia; 4Department of Cardiology, Dubrava University Hospital, Zagreb, Croatia; 5Faculty of Dental Medicine and Health, Josip Juraj Strossmayer University of Osijek, Osijek, Croatia.
Acta Clin Croat. 2019 Mar;58(1):57-62. doi: 10.20471/acc.2019.58.01.08.
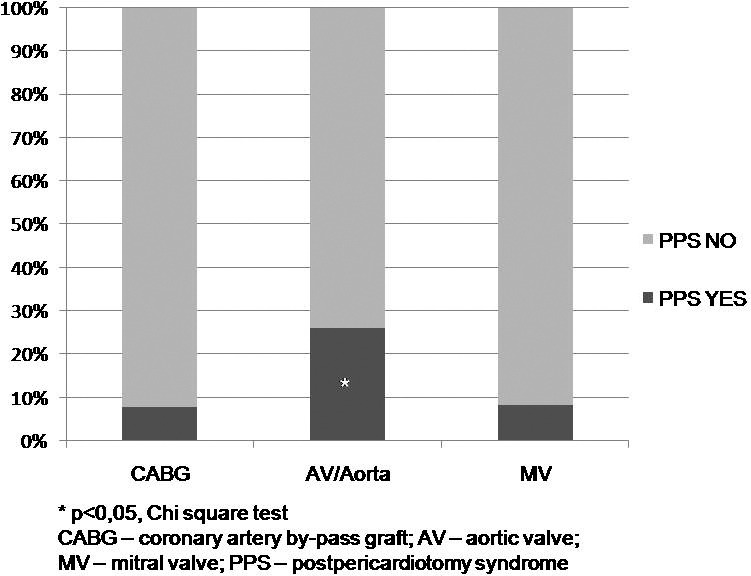
Postpericardiotomy syndrome (PPS) is worsening or new formation of pericardial and/or pleural effusion mostly 1 to 6 weeks after cardiac surgery, as a result of autoimmune inflammatory reaction within pleural and pericardial space. Its incidence varies among different studies and registries (2% to 30%), as well as according to the type of cardiac surgery performed. We conducted this retrospective analysis of PPS incidence and diagnostic and treatment strategies in patients referred for cardiac surgery for revascularization, valvular and/or aortic surgery. We retrospectively analyzed 461 patients referred for an urgent or elective cardiac surgery procedure between 2009 and 2015. PPS diagnosis was established using well defined clinical criteria. Demographic and clinical characteristics were used in regression subanalysis among patients having undergone surgery of aortic valve and/or ascending aorta. Within 6 weeks after cardiac surgery, 47 (10.2%) patients had PPS. The median time from the procedure to PPS diagnosis was 14 days. The incidence of PPS was 26% after aortic valve and/or aorta surgery, and 7.9% and 8.3% after coronary bypass and mitral valve surgery, respectively. Among patients subjected to aortic valve and/or aortic surgery, regression analysis showed significant association of fever, C-reactive protein (CRP) elevation between 5 and 100 mg/L, urgent procedure and postoperative antibiotic use with PPS diagnosis, whereas younger age showed near-significant association. All patients had complete resolution of PPS, mostly after corticosteroid therapy, with only 2 cases of recurrent PPS that successfully resolved after colchicine therapy. Pleural drainage was indicated in 15 (32%) patients, whereas only one patient required pericardial drainage. In conclusion, PPS incidence in our retrospective analysis was similar to previous reports. Patients having undergone aortic valve and/or aortic surgery were most likely to develop PPS. The most relevant clinical criteria for diagnosis in these patients were fever, CRP elevation between 5 and 100 mg/L, and pericardial and/or pleural effusion formation or worsening 2 weeks after cardiac surgery.
心包切开术后综合征(PPS)是指心脏手术后大多在1至6周出现的心包和/或胸腔积液的加重或新形成,这是胸腔和心包腔内自身免疫性炎症反应的结果。其发病率在不同研究和登记处有所不同(2%至30%),也因所进行的心脏手术类型而异。我们对因血管重建、瓣膜和/或主动脉手术而接受心脏手术的患者的PPS发病率及诊断和治疗策略进行了这项回顾性分析。我们回顾性分析了2009年至2015年间因紧急或择期心脏手术而转诊的461例患者。PPS诊断依据明确的临床标准确定。在接受主动脉瓣和/或升主动脉手术的患者中,人口统计学和临床特征用于回归亚分析。心脏手术后6周内,47例(10.2%)患者发生PPS。从手术到PPS诊断的中位时间为14天。主动脉瓣和/或主动脉手术后PPS的发病率为26%,冠状动脉搭桥术和二尖瓣手术后分别为7.9%和8.3%。在接受主动脉瓣和/或主动脉手术的患者中,回归分析显示发热、5至100mg/L之间的C反应蛋白(CRP)升高、急诊手术和术后使用抗生素与PPS诊断显著相关,而年龄较小显示出接近显著的相关性。所有患者的PPS均完全缓解,大多在使用皮质类固醇治疗后,只有2例复发性PPS在使用秋水仙碱治疗后成功缓解。15例(32%)患者需要胸腔引流,而只有1例患者需要心包引流。总之,我们回顾性分析中的PPS发病率与先前报告相似。接受主动脉瓣和/或主动脉手术的患者最易发生PPS。这些患者最相关的诊断临床标准是发热、5至100mg/L之间的CRP升高以及心脏手术后2周心包和/或胸腔积液形成或加重。