Khan Nayel, Clemens Mark, Liu Jun, Garden Adam S, Lawyer Anne, Weber Randal, Gunn G Brandon, Morrison William H, Kupferman Michael E
1Baylor College of Medicine, Houston, TX USA.
2Department of Plastic Surgery, University of Texas M. D. Anderson Cancer Center, Houston, TX USA.
Cancers Head Neck. 2019 Jul 22;4:4. doi: 10.1186/s41199-019-0043-2. eCollection 2019.
The optimal treatment for regional lymphatic recurrences from head and neck cancer has not been fully established. In order to explore the therapeutic benefit of surgical resection and adjuvant brachytherapy, the authors reviewed their experience utilizing interstitial brachytherapy (IBT) at the M. D. Anderson Cancer Center.
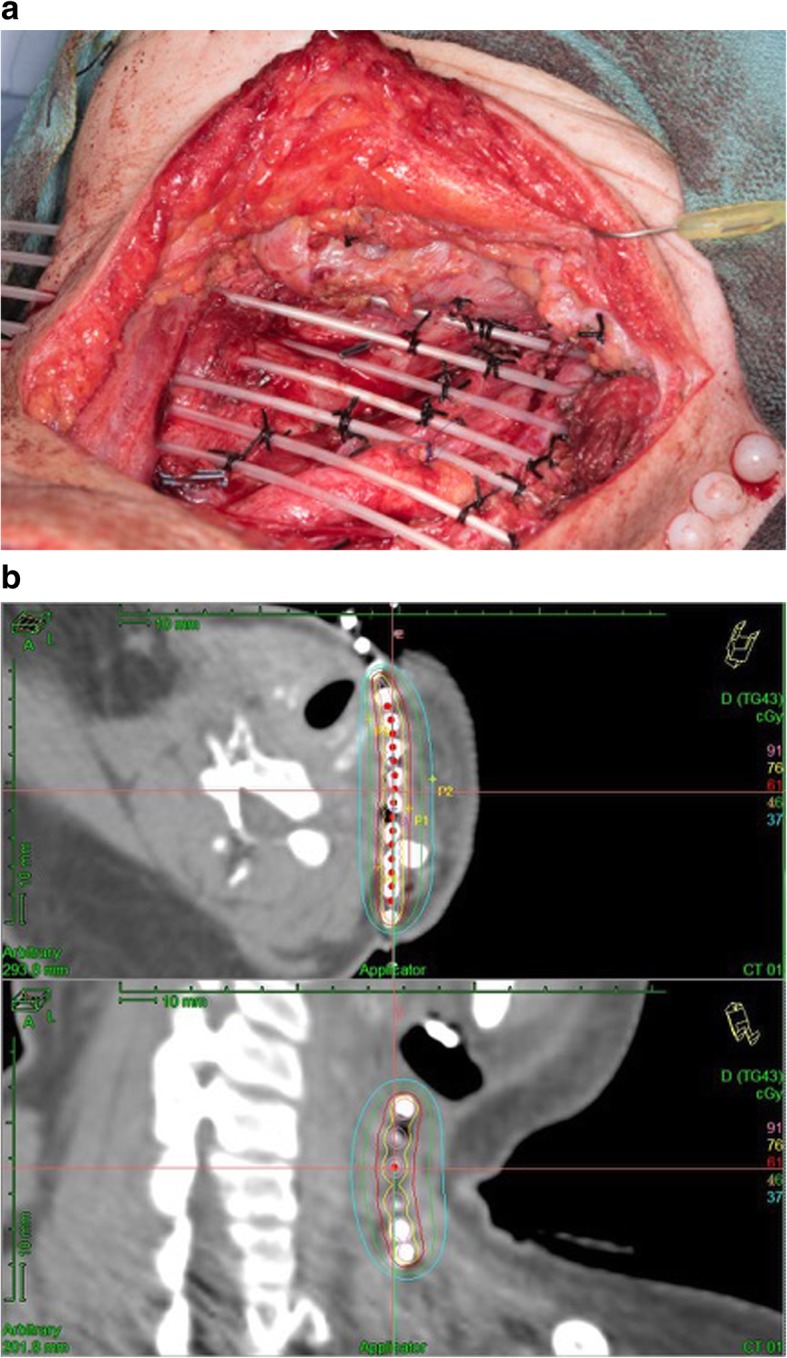
A retrospective chart review of the 51 patients who received salvage surgical resection of lymphatic recurrences and adjuvant IBT between 1993 and 2012 at the M. D. Anderson Cancer Center was undertaken. All patients underwent neck dissection with complete resection and intraoperative placement of afterloading brachytherapy catheters. Soft tissue reconstruction was performed as necessary. The technical aspects of IBT were reviewed, and the overall and disease free survival rates and the recurrence rates were determined.
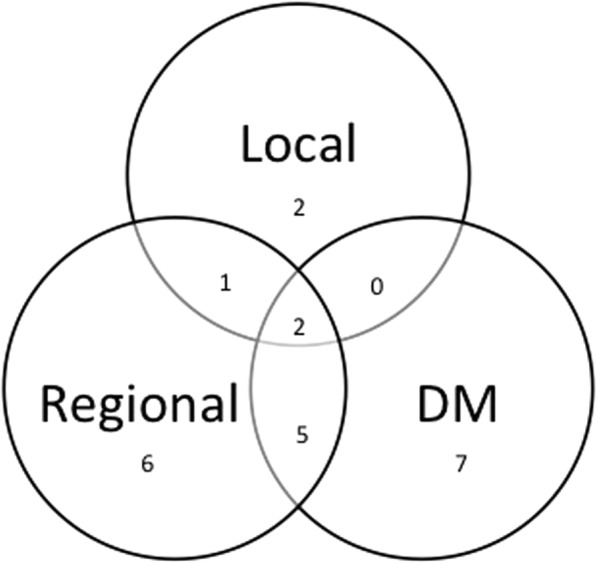
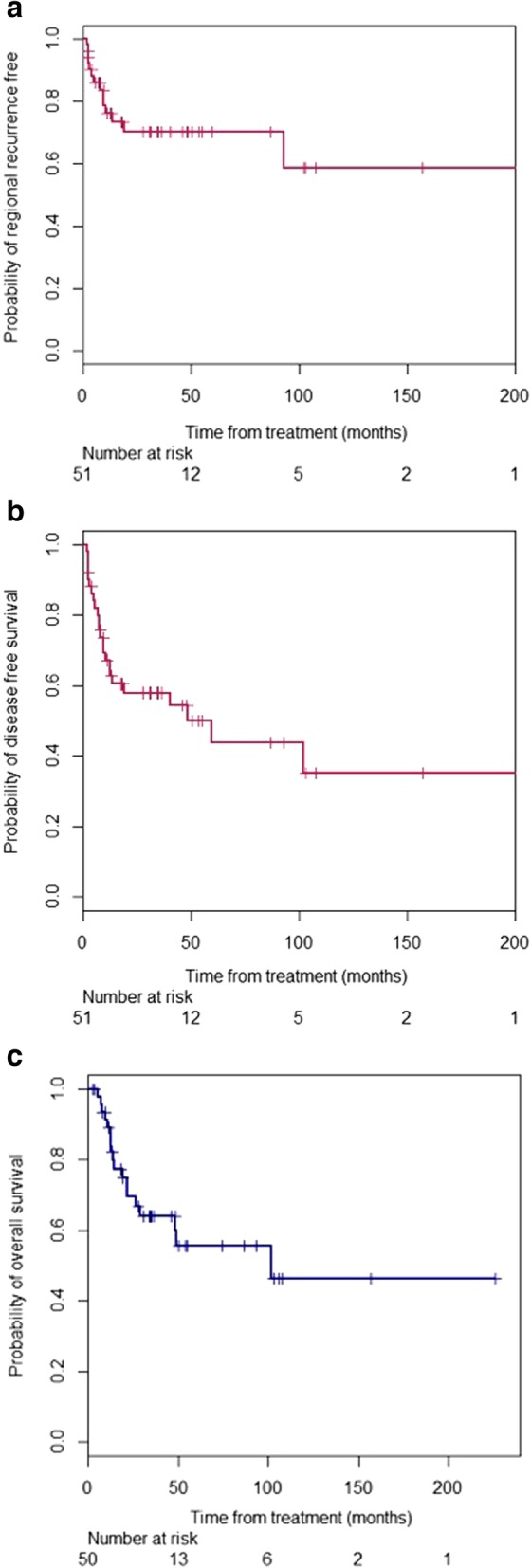
All patients had received external beam radiation (EBRT) as part of their initial treatment to a median dose of 66 Gy; 40 and 68% of the patients also had a neck dissection or chemotherapy, respectively. The cumulative regional recurrence probability is 28 and 38% at 5 years and 10 years. All of the patients underwent salvage neck dissection and IBT, with 81% also undergoing soft tissue reconstruction. The median dose delivered to the tumor bed was 60 Gy over a median duration of 4.5 days. There were 21 early adverse events, 8 of which were severe, and 19 late adverse events, 6 of which were severe. The most common early and late adverse events due to surgery and brachytherapy were dysphagia (7.1%) and true vocal cord paralysis (17.9%), respectively. There were no perioperative deaths or carotid hemorrhages. Nineteen patients developed recurrence including regional recurrence and distinct metastasis. The median time to recurrence is 130 months using Kaplan-Meier product limit method. The 2-year disease-free survival rate was 58%. The 2-year, 5-year, and 10-year overall survival rates were 69, 56, and 46%, respectively.
Regional recurrences in previously irradiated tissues after the definitive treatment of primary head and neck cancers represent a challenging problem. We demonstrated that salvage neck dissection with IBT provided encouraging regional control and survival rates, while maintaining relatively low acute and long-term toxicity rates.
头颈部癌区域淋巴结复发的最佳治疗方法尚未完全确立。为了探讨手术切除和辅助近距离放射治疗的治疗效果,作者回顾了他们在MD安德森癌症中心使用组织间近距离放射治疗(IBT)的经验。
对1993年至2012年期间在MD安德森癌症中心接受挽救性手术切除淋巴结复发并辅助IBT的51例患者进行回顾性病历审查。所有患者均接受颈部清扫术,完整切除并在术中放置后装近距离放射治疗导管。必要时进行软组织重建。回顾了IBT的技术方面,并确定了总生存率、无病生存率和复发率。
所有患者在初始治疗中均接受了外照射放疗(EBRT),中位剂量为66Gy;分别有40%和68%的患者还进行了颈部清扫或化疗。5年和10年时区域复发累积概率分别为28%和38%。所有患者均接受了挽救性颈部清扫和IBT,81%的患者还进行了软组织重建。肿瘤床的中位剂量为60Gy,中位持续时间为4.5天。有21例早期不良事件,其中8例严重,19例晚期不良事件,其中6例严重。手术和近距离放射治疗最常见的早期和晚期不良事件分别为吞咽困难(7.1%)和真性声带麻痹(17.9%)。无围手术期死亡或颈动脉出血。19例患者出现复发,包括区域复发和远处转移。使用Kaplan-Meier乘积限界法得出的复发中位时间为130个月。2年无病生存率为58%。2年、5年和10年总生存率分别为69%、56%和46%。
原发性头颈部癌根治性治疗后先前照射组织中的区域复发是一个具有挑战性的问题。我们证明,挽救性颈部清扫联合IBT可提供令人鼓舞的区域控制率和生存率,同时保持相对较低的急性和长期毒性率。