Division of Pulmonary and Critical Care Medicine, Boston, Mass; Applied Chest Imaging Laboratory, Brigham and Women's Hospital, Boston, Mass.
Department of Preventive Medicine, Northwestern University Feinberg School of Medicine, Chicago, Ill.
Am J Med. 2020 Feb;133(2):222-230.e11. doi: 10.1016/j.amjmed.2019.06.049. Epub 2019 Jul 29.
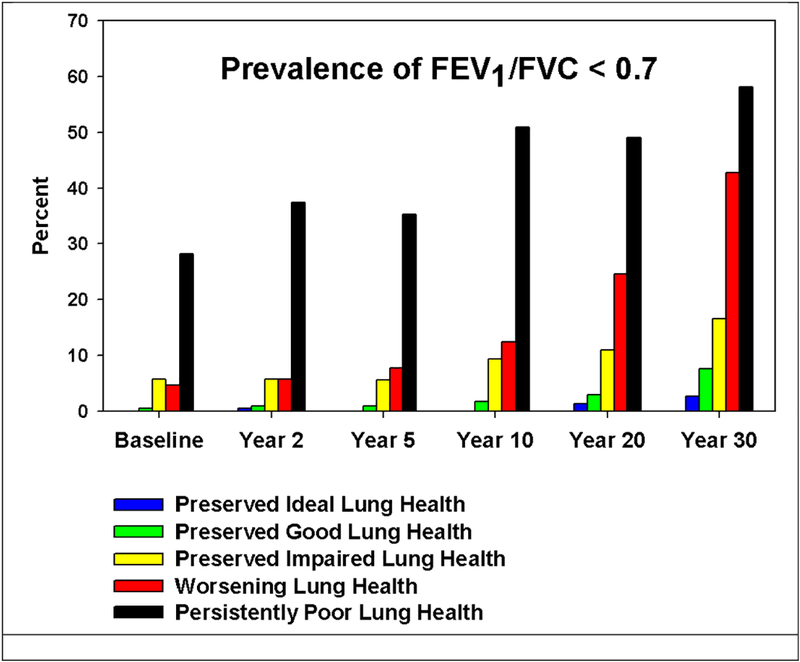
Peak lung function and rate of decline predict future airflow obstruction and nonrespiratory comorbid conditions. Associations between lung function trajectories and emphysema have not been explored.
Using data from the population-based CARDIA Study, we sought to describe the prevalence of visually ascertained emphysema at multiple time points and contextualize its development based upon participant's adult life course measures of lung function. There were 3171 men and women enrolled at a mean age of 25 years, who underwent serial spirometric examinations through a mean age of 55 years. Trajectories for the change in percent-predicted forced expiratory volume in one second (FEV) were determined by fitting a mixture model via maximum likelihood. Emphysema was visually identified on computed tomographic scans and its prevalence reported at mean ages of 40, 45, and 50 years.
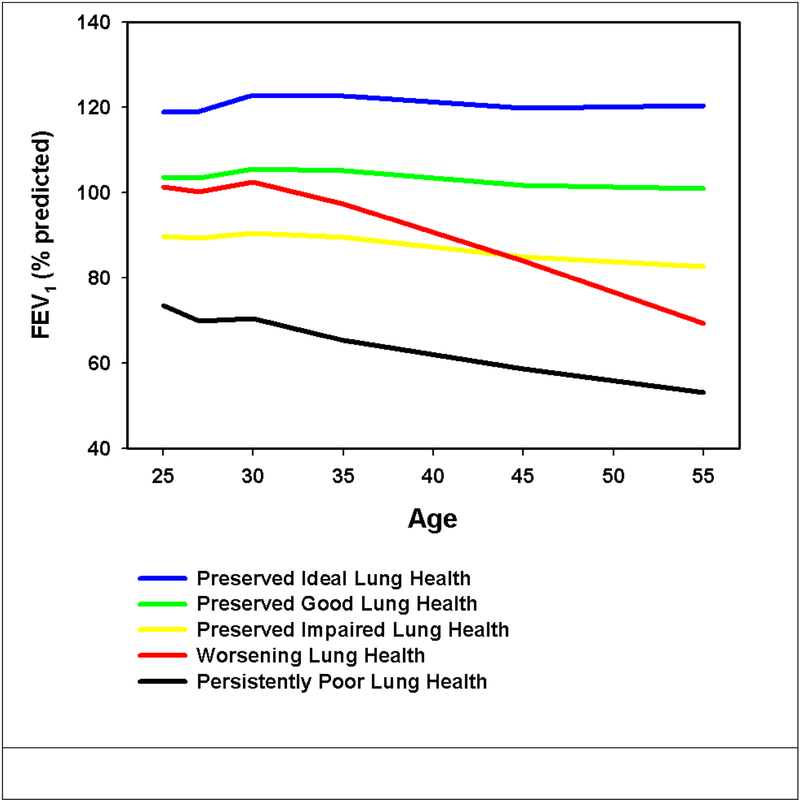
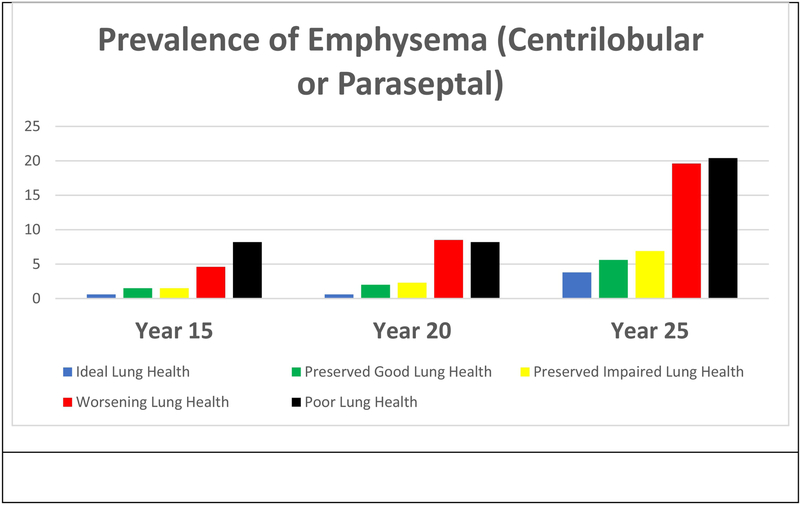
We identified 5 trajectories describing peak and change in FEV: "Preserved Ideal," "Preserved Good," "Preserved Impaired," "Worsening," and "Persistently Poor." Ever smokers comprised part of all 5 trajectories. The prevalence of emphysema was 1.7% (n = 46; mean age of 40 years), 2.5% (n = 67; mean age of 45 years), and 7.1% (n = 189; mean age of 50 years). Of those with emphysema at a mean age of 50 years, 18.0% were never smokers. Worsening and poor lung health trajectories were associated with increased odds of future emphysema independent of chronic tobacco smoke exposure (odds ratio 5.06; confidence interval, 1.84-13.96; odds ratio 4.85; confidence interval, 1.43-16.44).
Lower peak and accelerated decline in FEV are risk factors for future emphysema independent of smoking status.
肺功能峰值和下降速度可预测未来气流阻塞和非呼吸道合并症。肺功能轨迹与肺气肿之间的关联尚未得到探索。
使用基于人群的 CARDIA 研究的数据,我们试图描述在多个时间点通过视觉确定的肺气肿的患病率,并根据参与者的成年期肺功能测量值来确定其发展情况。共有 3171 名男性和女性在平均年龄为 25 岁时入组,他们在平均年龄为 55 岁时接受了连续的肺活量检查。通过最大似然法拟合混合模型来确定一秒用力呼气量(FEV)预计百分比变化的轨迹。在计算机断层扫描上识别肺气肿,并报告其在平均年龄为 40、45 和 50 岁时的患病率。
我们确定了描述 FEV 峰值和变化的 5 个轨迹:“理想保留”、“良好保留”、“保留受损”、“恶化”和“持续不良”。所有 5 个轨迹中都有吸烟者。肺气肿的患病率为 1.7%(n=46;平均年龄为 40 岁)、2.5%(n=67;平均年龄为 45 岁)和 7.1%(n=189;平均年龄为 50 岁)。在平均年龄为 50 岁时患有肺气肿的患者中,18.0%为从不吸烟者。恶化和不良的肺健康轨迹与未来肺气肿的发生几率增加独立相关,而与慢性烟草烟雾暴露无关(比值比 5.06;置信区间,1.84-13.96;比值比 4.85;置信区间,1.43-16.44)。
较低的 FEV 峰值和加速下降是未来肺气肿的危险因素,与吸烟状况无关。