Section for Sustainable Health.
Department of Public Health and Clinical Medicine, and.
Am J Respir Crit Care Med. 2023 Nov 15;208(10):1063-1074. doi: 10.1164/rccm.202211-2166OC.
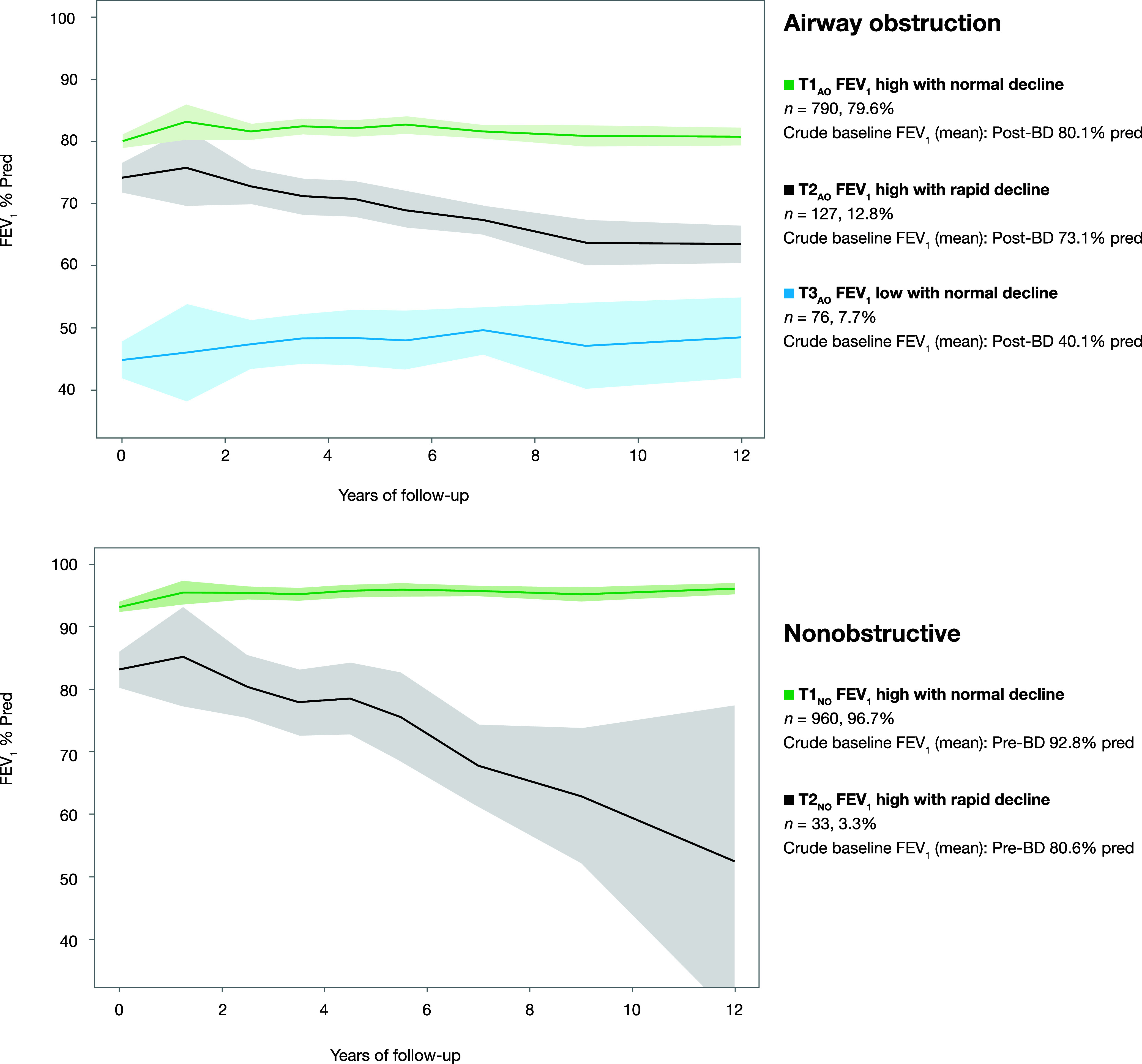
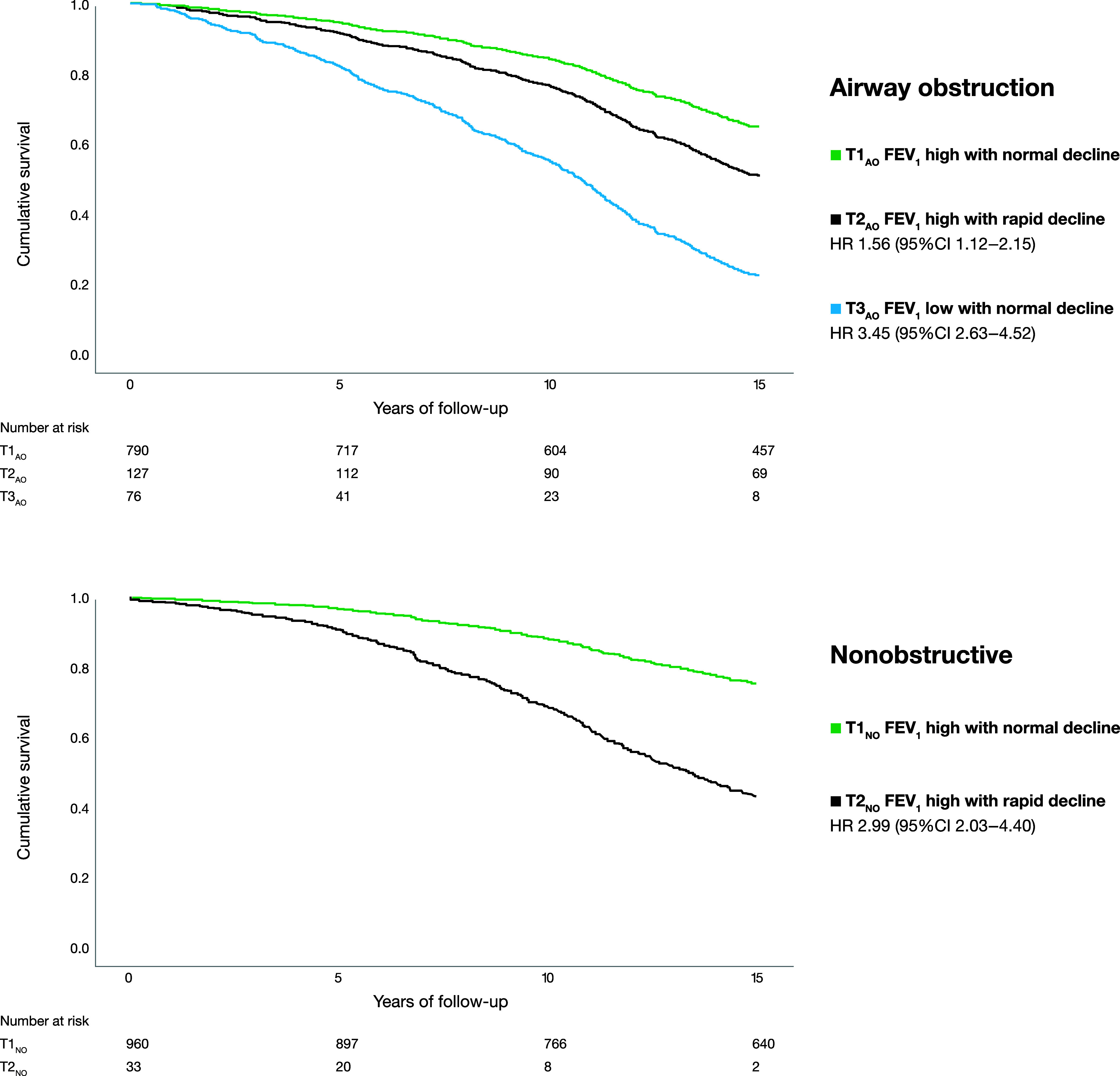
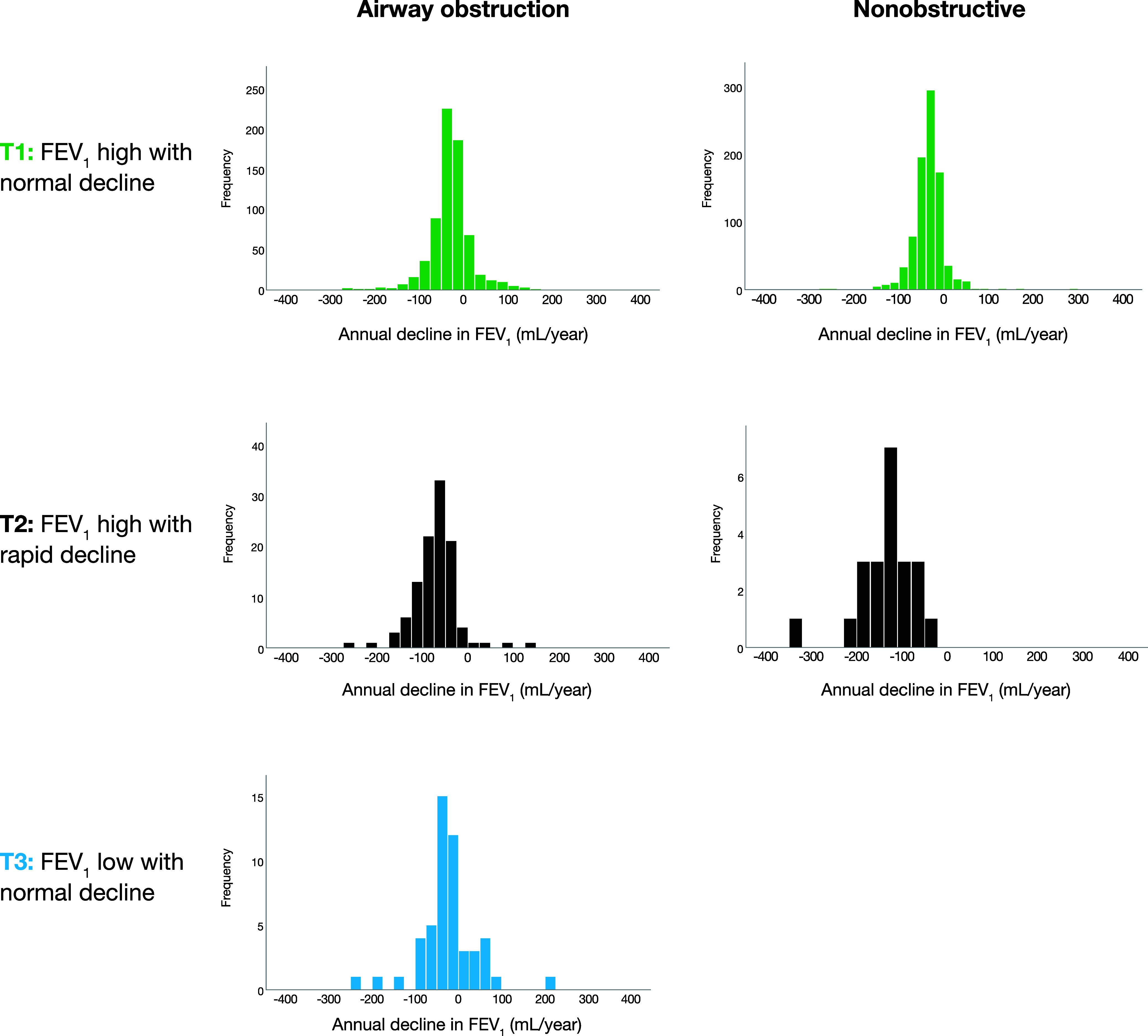
Spirometry is essential for diagnosis and assessment of prognosis in patients with chronic obstructive pulmonary disease (COPD). To identify FEV trajectories and their determinants on the basis of annual spirometry measurements among individuals with and without airway obstruction (AO) and to assess mortality in relation to trajectories. From 2002 through 2004, individuals with AO (FEV/VC < 0.70, = 993) and age- and sex-matched nonobstructive (NO) referents were recruited from population-based cohorts. Annual spirometry until 2014 was used in joint-survival latent-class mixed models to identify lung function trajectories. Mortality data were collected during 15 years of follow-up. Three trajectories were identified among the subjects with AO and two among the NO referents. Trajectory membership was driven by baseline FEV% predicted (FEV%pred) in both groups and also by pack-years in subjects with AO and current smoking in NO referents. Longitudinal FEV%pred depended on baseline FEV%pred, pack-years, and obesity. The trajectories were distributed as follows: among individuals with AO, 79.6% in AO trajectory 1 (FEV high with normal decline), 12.8% in AO trajectory 2 (FEV high with rapid decline), and 7.7% in AO trajectory 3 (FEV low with normal decline) (mean, 27, 72, and 26 ml/yr, respectively) and, among NO referents, 96.7% in NO trajectory 1 (FEV high with normal decline) and 3.3% in NO trajectory 2 (FEV high with rapid decline) (mean, 34 and 173 ml/yr, respectively). Hazard for death was increased for AO trajectories 2 (hazard ratio [HR], 1.56) and 3 (HR, 3.45) versus AO trajectory 1 and for NO trajectory 2 (HR, 2.99) versus NO trajectory 1. Three different FEV trajectories were identified among subjects with AO and two among NO referents, with different outcomes in terms of FEV decline and mortality. The FEV trajectories among subjects with AO and the relationship between low FVC and trajectory outcome are of particular clinical interest.
肺量测定对于慢性阻塞性肺疾病(COPD)患者的诊断和预后评估至关重要。本研究旨在通过对存在和不存在气道阻塞(AO)的个体进行年度肺量测定,确定基于肺功能的轨迹及其决定因素,并评估与轨迹相关的死亡率。从 2002 年至 2004 年,从基于人群的队列中招募了 AO 患者(FEV/VC < 0.70,= 993)和年龄、性别匹配的非阻塞性(NO)对照者。在 15 年的随访期间,使用年度肺量测定来收集死亡率数据。在存在 AO 的受试者和不存在 AO 的对照者中,使用联合生存潜在类别混合模型确定了肺功能轨迹。在存在 AO 的受试者和不存在 AO 的对照者中,分别确定了 3 个和 2 个轨迹。两组的轨迹成员资格都取决于基线时的 FEV%预测值(FEV%pred),并且还取决于存在 AO 的受试者的吸烟包年数和不存在 AO 的对照者的当前吸烟状况。纵向 FEV%pred 取决于基线时的 FEV%pred、吸烟包年数和肥胖。轨迹分布如下:在存在 AO 的个体中,AO 轨迹 1(FEV 高且正常下降)占 79.6%,AO 轨迹 2(FEV 高且快速下降)占 12.8%,AO 轨迹 3(FEV 低且正常下降)占 7.7%(平均分别为 27、72 和 26ml/yr);在不存在 AO 的对照者中,NO 轨迹 1(FEV 高且正常下降)占 96.7%,NO 轨迹 2(FEV 高且快速下降)占 3.3%(平均分别为 34 和 173ml/yr)。与 AO 轨迹 1 相比,AO 轨迹 2(危险比[HR],1.56)和 3(HR,3.45)的死亡风险增加,与 NO 轨迹 1 相比,NO 轨迹 2(HR,2.99)的死亡风险增加。在存在 AO 的个体中确定了 3 种不同的 FEV 轨迹,在不存在 AO 的对照者中确定了 2 种不同的 FEV 轨迹,FEV 下降和死亡率的结果也不同。存在 AO 的个体的 FEV 轨迹以及 FVC 低值与轨迹结果之间的关系具有特殊的临床意义。