CISM (Centro de Investigação em Saúde de Manhiça), Bairro Cambeve, Rua 12, Distrito da Manhiça, Maputo, CP 1929, Mozambique.
ISGlobal, Hospital Clínic, Universitat de Barcelona, Barcelona, Spain.
BMC Public Health. 2019 Aug 1;19(1):1031. doi: 10.1186/s12889-019-7338-4.
In Mozambique cervical cancer is a public health threat, due to its high incidence and limited access to early diagnosis of precancerous lesions. International organisations are supporting the introduction of human papillomavirus (HPV) vaccines in low- and middle-income countries. Some of these countries recently conducted demonstration programmes, which included evaluation of acceptability, coverage, and practicality of implementation and of integration in existing programmes. Information on costs of delivering the vaccine is needed to overcome the challenges of reaching vaccine potential recipients in rural and remote areas.
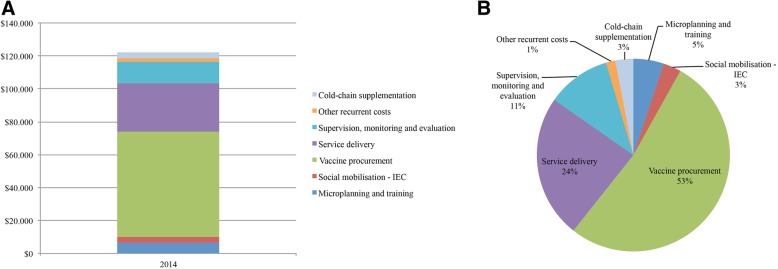
We estimated the financial and economic costs of delivering HPV vaccination to ten-year-old girls at schools for the first vaccination cycle of the demonstration programme in the Manhiça district (southern Mozambique), delivered throughout 2014. We also estimated costs of an alternative scenario with a reduced number of doses and personnel, which was analogous to the second vaccination cycle delivered throughout 2015. Cost estimates followed a micro-costing approach and included interviews with key informants at different administrative levels through the administration of standard questionnaires developed by the World Health Organisation.
Considering only data from the first vaccination cycle (2014), which consisted in the administration of three doses, the average economic cost was US$17.59 per dose and US$52.29 per fully-immunised girl (FIG). Financial cost per dose (US$6.07) and per FIG (US$17.95) were substantially lower. The economic cost was US$15.53 per dose and US$31.14 per FIG when estimating an alternative cost scenario with reduced number of doses and personnel.
The average economic cost per dose was lower than the ones recently reported for low- and middle-income countries. However, our estimation of the financial cost per FIG was higher than the ones observed elsewhere (ranging from US$2.49 in India to US$20.36 in Vietnam) due to the high percentage of out-of-school girls which, reduced vaccine coverage and, therefore, reduced the denominator. Due to budget constraints, if Mozambique is to implement nation-wide HPV vaccination targeted to ten-year-old girls at schools, a reduction in personnel costs should be operated either by restricting the outreach vaccinator team or the number of supervision visits.
在莫桑比克,宫颈癌是一个公共卫生威胁,因为其发病率高,而且难以早期诊断癌前病变。国际组织正在支持在低收入和中等收入国家引入人乳头瘤病毒(HPV)疫苗。其中一些国家最近开展了示范项目,包括评估可接受性、覆盖率和实施的实用性,以及与现有方案的整合。需要了解提供疫苗的成本信息,以克服在农村和偏远地区为疫苗潜在受种者提供疫苗的挑战。
我们估计了在马希奇区(莫桑比克南部)学校为 10 岁女孩提供 HPV 疫苗接种的第一个周期(示范项目)的财务和经济成本,该周期在 2014 年全年进行。我们还估计了减少剂量和人员的替代方案的成本,该方案类似于 2015 年全年进行的第二个周期。成本估计采用微观成本核算方法,包括通过世界卫生组织制定的标准问卷,对不同行政级别的关键信息员进行访谈。
仅考虑第一个周期(2014 年)的数据,即接种三剂疫苗,每剂疫苗的平均经济成本为 17.59 美元,每例完全免疫女孩(FIG)为 52.29 美元。每剂疫苗的财务成本(6.07 美元)和每例 FIG(17.95 美元)要低得多。当估计剂量和人员减少的替代成本方案时,每剂的经济成本为 15.53 美元,每例 FIG 为 31.14 美元。
每剂疫苗的平均经济成本低于最近报告的低收入和中等收入国家的成本。然而,我们对每例 FIG 的财务成本的估计高于其他地方观察到的成本(从印度的 2.49 美元到越南的 20.36 美元不等),因为失学女孩的比例很高,这降低了疫苗的覆盖率,因此降低了分母。由于预算限制,如果莫桑比克要在全国范围内针对在校 10 岁女孩实施 HPV 疫苗接种,应通过限制外展疫苗接种团队或监督访问次数来降低人员成本。