Naeem Bilqis, Moorani Khemchand N, Anjum Misbah, Imam Uzma
Bilquis Naeem, MBBS, FCPS, FCPS, Assistant Professor, Pediatric Medicine, Departments of Pediatric Nephrology, National Institute of Child Health (NICH), Jinnah Sindh Medical University (JSMU) Karachi, Pakistan.
Prof. Khemchand N Moorani, FCPS, MCPS, MBBS, Departments of Pediatric Nephrology, National Institute of Child Health (NICH), Jinnah Sindh Medical University (JSMU) Karachi, Pakistan.
Pak J Med Sci. 2019 Jul-Aug;35(4):899-904. doi: 10.12669/pjms.35.4.715.
Tumor lysis syndrome (TLS) is common complication of acute lymphoblastic leukemia (ALL). It is characterized by presence of two or more of hyperkalemia, hyperuricemia, hyperphosphatemia and hypocalcemia. TLS may cause acute kidney injury (AKI), arrhythmias and seizures. Our objective was to determine the frequency of TLS and its biochemical abnormalities in children with ALL.
A retrospective study on 91 children, aged 2-13 years with ALL was carried out in Nephrology and Oncology departments of National Institute of Child Health, Karachi from January 2016 to December 2017. Patients already received chemotherapy were excluded. Data including risk categories, immunophenotyping, laboratory parameters like complete blood picture, serum creatinine (SCr), potassium(K), calcium (Ca), phosphorus(P) and uric acid (UA) on day 0,3 and 7 after chemotherapy were collected. Data analyzed on SPSS using descriptive statistics. Independent t- test was applied to compare means and P- value<0.05 was taken as significant.
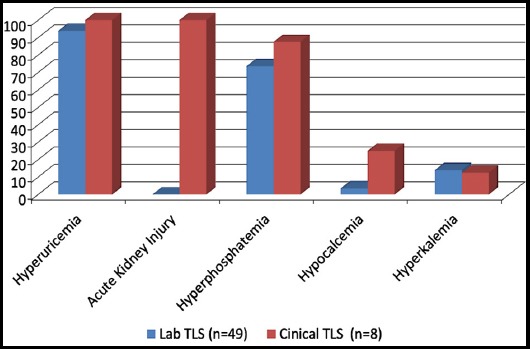
Ninety-one children with mean age of 6.39±3.08 years were studied. Male were 57% and 43% female. High risk ALL were 61.5%. Pre -BALL were 82.4% and 17.5% had T-cell ALL. All patients had anemia (hemoglobin7.69±2.66 g/dl) and thrombocytopenia (43.61± 18.6 x10) where as hyperleukocytosis and blast cells were observed in 20.87% and 73.6% respectively. Comparing the biochemical parameters of ALL, the difference in SCr from D0 vs D3 (0.46±0.16 vs0.54± 0.35 and D7, 0.44±0.22) was significant (p=0.001). Similarly, difference in UA (D0, 4.12±2.40 vs D3, 3.82±1.73 and D7, 3.56±1.42), SP (D0, 4.24±1.34 vs D3, 4.61±1.76 and D7,4.13±1.07mg/dl)and for K (p=0.038) was significant. There was no difference in Ca from D0 vs D3 (0.092) and D7 (0.277). TLS was found in 62.6% children, it was chemotherapy induced in 72% and spontaneous in 28%. Clinical-TLS was observed in 14% and all CTLS had AKI. Hyperuricemia and hyperphosphatemia were the most common biochemical abnormalities in laboratory-TLS and CTLS.
TLS was found in 62.6% despite preventive measures. Early recognition and treatment is essential to avoid morbidity and mortality.
肿瘤溶解综合征(TLS)是急性淋巴细胞白血病(ALL)的常见并发症。其特征为存在高钾血症、高尿酸血症、高磷血症和低钙血症中的两种或更多种。TLS可能导致急性肾损伤(AKI)、心律失常和癫痫发作。我们的目的是确定ALL患儿中TLS及其生化异常的发生率。
2016年1月至2017年12月在卡拉奇国家儿童健康研究所的肾脏病科和肿瘤科对91名年龄在2至13岁的ALL患儿进行了一项回顾性研究。已接受化疗的患者被排除。收集包括风险类别、免疫表型分析、化疗后第0、3和7天的实验室参数,如全血细胞计数、血清肌酐(SCr)、钾(K)、钙(Ca)、磷(P)和尿酸(UA)。使用描述性统计方法在SPSS上对数据进行分析。应用独立t检验比较均值,P值<0.05被视为具有显著性。
研究了91名平均年龄为6.39±3.08岁的儿童。男性占57%,女性占43%。高危ALL占61.5%。前B细胞ALL占82.4%,17.5%为T细胞ALL。所有患者均有贫血(血红蛋白7.69±2.66 g/dl)和血小板减少(43.61±18.6×10),而分别有20.87%和73.6%的患者出现白细胞增多和原始细胞。比较ALL的生化参数,化疗第0天与第3天(0.46±0.16对0.54±0.35)以及第7天(0.44±0.22)的SCr差异具有显著性(p = 0.001)。同样,尿酸(第0天,4.12±2.40对第3天,3.82±1.73和第7天,3.56±1.42)、磷(第0天,4.24±1.34对第3天,4.61±1.76和第7天,4.13±1.07mg/dl)以及钾(p = 0.038)的差异具有显著性。化疗第0天与第3天(0.092)以及第7天(0.277)的钙无差异。62.6%的儿童发现有TLS,其中72%为化疗诱导型,28%为自发型。14%观察到临床TLS,所有临床TLS患者均有AKI。高尿酸血症和高磷血症是实验室TLS和临床TLS中最常见的生化异常。
尽管采取了预防措施,仍有62.6%的患者出现TLS。早期识别和治疗对于避免发病和死亡至关重要。