Department of Surgery, Clinical Sciences Lund, Lund University and Skåne University Hospital, SE-221 85, Lund, Sweden.
Langenbecks Arch Surg. 2019 Aug;404(5):565-571. doi: 10.1007/s00423-019-01810-0. Epub 2019 Aug 3.
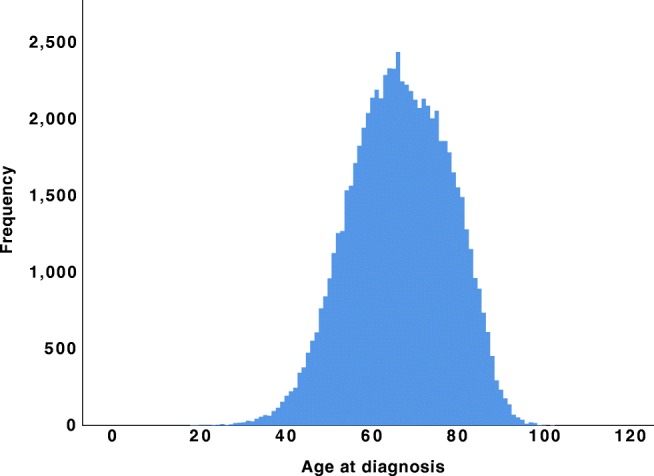
Early-onset pancreatic cancer (< 50 years, EOPC) is uncommon and limited data exist on clinical presentation and long-term survival. The aim of this study was to compare outcomes between patients with EOPC and those with later-onset pancreatic cancer (≥ 50 years, LOPC) using a large population-based cohort.
The Surveillance, Epidemiology, and End Results (SEER) database was queried to identify patients with a microscopically confirmed pancreatic ductal adenocarcinoma for the period 2004 to 2016. Propensity score matching was used to compare overall survival (OS) and cancer-specific survival (CSS) between patients with EOPC and LOPC. The EOPC and LOPC patients were paired 1:1 on propensity scores based on gender, tumor location, tumor size, AJCC stage, and treatment details.
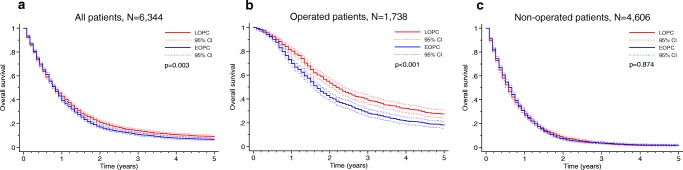
The overall cohort included 72,906 patients with pancreatic ductal adenocarcinoma, including 4523 patients with EOPC (6.2%). EOPC patients were diagnosed at a more advanced AJCC stage (p < 0.001) compared with LOPC patients and received significantly more treatment, including surgery (p < 0.001), radiation (p < 0.001), and chemotherapy (p < 0.001). Following propensity score matching, 3172 EOPC patients were matched to 3172 LOPC patients, alleviating any covariate differences between the groups. The matched analysis showed that EOPC was associated with poorer 5-year OS (6.1% vs 8.6%, p = 0.003) and 5-year CSS (6.7% vs 9.7%, p < 0.001). In multivariable Cox regression analysis, EOPC remained significantly associated with adverse OS and CSS. Subgroup analyses showed that EOPC was associated with adverse 5-year OS (17.7% vs 26.9%, p < 0.001) and 5-year CSS (18.9% vs 29.7%, p < 0.001) in operated patients. After multivariable analysis, EOPC remained significantly associated with OS and CSS. For patients that did not undergo surgery, the OS and CSS remained dismal without any significant differences between the groups.
To our knowledge, this is the largest study to compare the outcome of EOPC vs LOPC, as well as the first to use propensity score matching methodology for this purpose. The findings demonstrate that EOPC is diagnosed at a later stage and the matched survival analysis demonstrated reduced OS and CSS. We suggest that pancreatic cancer in young patients may have a unique tumor biology, which may be of importance for risk stratification and patient counseling.
早发性胰腺癌(<50 岁,EOPC)较为少见,目前关于其临床表现和长期生存的数据有限。本研究旨在使用大型人群队列比较 EOPC 患者和晚发性胰腺癌(≥50 岁,LOPC)患者的结局。
通过监测、流行病学和最终结果(SEER)数据库,确定 2004 年至 2016 年间显微镜下确诊为胰腺导管腺癌的患者。使用倾向评分匹配比较 EOPC 和 LOPC 患者的总生存期(OS)和癌症特异性生存期(CSS)。EOPC 和 LOPC 患者根据性别、肿瘤位置、肿瘤大小、AJCC 分期和治疗细节,基于倾向评分以 1:1 的比例配对。
总体队列包括 72906 名胰腺导管腺癌患者,其中 4523 名(6.2%)为 EOPC 患者。与 LOPC 患者相比,EOPC 患者的 AJCC 分期更晚(p<0.001),并且接受了更多的治疗,包括手术(p<0.001)、放疗(p<0.001)和化疗(p<0.001)。在进行倾向评分匹配后,3172 名 EOPC 患者与 3172 名 LOPC 患者匹配,缓解了两组之间的任何协变量差异。匹配分析显示,EOPC 与较差的 5 年 OS(6.1% vs 8.6%,p=0.003)和 5 年 CSS(6.7% vs 9.7%,p<0.001)相关。多变量 Cox 回归分析显示,EOPC 与不良 OS 和 CSS 显著相关。亚组分析显示,在接受手术的患者中,EOPC 与较差的 5 年 OS(17.7% vs 26.9%,p<0.001)和 5 年 CSS(18.9% vs 29.7%,p<0.001)相关。在多变量分析后,EOPC 与 OS 和 CSS 仍显著相关。对于未接受手术的患者,两组之间的 OS 和 CSS 仍然很差,没有显著差异。
据我们所知,这是最大的比较 EOPC 与 LOPC 结局的研究,也是首次使用倾向评分匹配方法进行此类研究。研究结果表明,EOPC 诊断较晚,匹配生存分析显示 OS 和 CSS 降低。我们建议,年轻患者的胰腺癌可能具有独特的肿瘤生物学特性,这可能对风险分层和患者咨询具有重要意义。