From the Department of Medicine, University of California San Francisco (A.K.L., V.J., M.G.S.).
Division of Nephrology, University of Washington, Seattle (R.K.).
Hypertension. 2019 Oct;74(4):872-879. doi: 10.1161/HYPERTENSIONAHA.119.13339. Epub 2019 Aug 5.
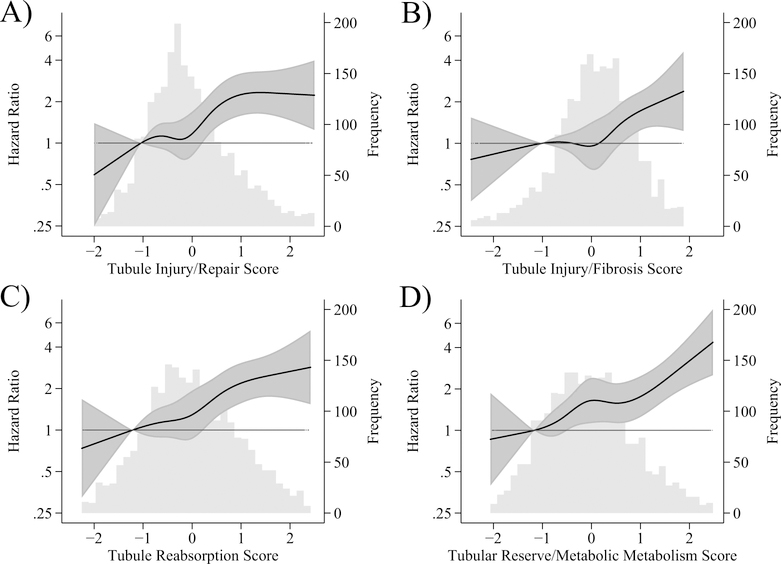
Chronic kidney disease is a strong risk factor for cardiovascular disease (CVD), but clinical kidney measures (estimated glomerular filtration rate and albuminuria) do not fully reflect the multiple aspects of kidney tubules influencing cardiovascular health. Applied methods are needed to integrate numerous tubule biomarkers into useful prognostic scores. In SPRINT (Systolic Blood Pressure Intervention Trial) participants with chronic kidney disease at baseline (estimated glomerular filtration rate <60 mL/minute per 1.73 m), we measured 8 biomarkers from urine (α1M [α1M microglobulin], β2M [β2M microglobulin], umod [uromodulin], KIM-1 [kidney injury molecule-1], MCP-1 [monocyte chemoattractant protein-1], YKL-40 [chitinase-3-like protein-1], NGAL [neutrophil gelatinase-associated lipocalin], and IL-18 [interleukin 18]) and 2 biomarkers from serum (intact parathyroid hormone, iFGF-23 [intact fibroblast growth factor-23]). We used an unsupervised method, exploratory factor analysis, to create summary scores of tubule health dimensions. Adjusted Cox models evaluated each tubule score with CVD events, heart failure, and all-cause mortality. We examined CVD discrimination using Harrell C-statistic. Factor analysis of 10 biomarkers from 2376 SPRINT-chronic kidney disease participants identified 4 unique dimensions of tubular health: tubule injury/repair (NGAL, IL-18, YKL-40), tubule injury/fibrosis (KIM-1, MCP-1), tubule reabsorption (α1M, β2M), and tubular reserve/mineral metabolism (umod, intact parathyroid hormone, iFGF-23). After adjustment for CVD risk factors, estimated glomerular filtration rate, and albumin-to-creatinine ratio, 2 of the 4 tubule scores were associated with CVD (hazard ratio per SD; reabsorption, 1.21 [1.06-1.38]; reserve, 1.24 (1.08-1.38]), 1 with heart failure (reserve, 1.41 [1.13-1.74]), and none with mortality. Compared with a base model (C-statistic=0.674), adding estimated glomerular filtration rate and albumin-to-creatinine ratio improved the C-statistic (C=0.704; =0.001); further adding tubule scores additionally improved the C-statistic (C=0.719; =0.009). In the setting of chronic kidney disease, dimensions of tubule health quantified using factor analysis improved CVD discrimination beyond contemporary kidney measures. Clinical Trial Registration- URL: http://www.clinicaltrials.gov. Unique identifier: NCT01206062.
慢性肾脏病是心血管疾病(CVD)的一个强有力的危险因素,但临床肾脏指标(估计肾小球滤过率和白蛋白尿)并不能完全反映影响心血管健康的多个肾小管方面。需要应用方法将众多肾小管生物标志物整合到有用的预后评分中。在 SPRINT(收缩压干预试验)中,基线时患有慢性肾脏病的患者(估计肾小球滤过率<60mL/min/1.73m),我们测量了 8 种来自尿液的生物标志物(α1M[α1M 微球蛋白]、β2M[β2M 微球蛋白]、umod[尿调蛋白]、KIM-1[肾损伤分子-1]、MCP-1[单核细胞趋化蛋白-1]、YKL-40[壳多糖酶 3 样蛋白-1]、NGAL[中性粒细胞明胶酶相关脂质运载蛋白]和 IL-18[白细胞介素 18])和 2 种来自血清的生物标志物(完整甲状旁腺激素,iFGF-23[完整成纤维细胞生长因子 23])。我们使用无监督方法,探索性因子分析,创建肾小管健康维度的综合评分。调整后的 Cox 模型用 CVD 事件、心力衰竭和全因死亡率评估每个肾小管评分。我们使用 Harrell C 统计量评估 CVD 区分度。对来自 2376 名 SPRINT-慢性肾脏病患者的 10 种生物标志物进行因子分析,确定了肾小管健康的 4 个独特维度:肾小管损伤/修复(NGAL、IL-18、YKL-40)、肾小管损伤/纤维化(KIM-1、MCP-1)、肾小管重吸收(α1M、β2M)和肾小管储备/矿物质代谢(umod、完整甲状旁腺激素、iFGF-23)。在调整 CVD 风险因素、估计肾小球滤过率和白蛋白与肌酐比值后,4 个肾小管评分中的 2 个与 CVD 相关(每标准差的风险比;重吸收,1.21[1.06-1.38];储备,1.24[1.08-1.38]),1 个与心力衰竭相关(储备,1.41[1.13-1.74]),没有与死亡率相关。与基础模型(C 统计量=0.674)相比,增加估计肾小球滤过率和白蛋白与肌酐比值可提高 C 统计量(C=0.704;=0.001);进一步增加肾小管评分可进一步提高 C 统计量(C=0.719;=0.009)。在慢性肾脏病患者中,使用因子分析定量的肾小管健康维度改善了 CVD 区分度,超过了当前的肾脏指标。临床试验注册- URL:http://www.clinicaltrials.gov。唯一标识符:NCT01206062。