Department of Surgery, Matsusaka Municipal Hospital, 1550, Tonomachi, Matsusaka, Mie, Japan.
Department of Gastroenterology, Matsusaka Municipal Hospital, 1550, Tonomachi, Matsusaka, Mie, Japan.
World J Surg Oncol. 2019 Aug 5;17(1):134. doi: 10.1186/s12957-019-1681-x.
Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) is a useful tool in pancreatic cancer diagnosis. However, the procedure itself may cause peritoneal dissemination and needle tract seeding at the puncture site. We herein report two cases of gastric wall metastasis due to needle tract seeding after EUS-FNA.
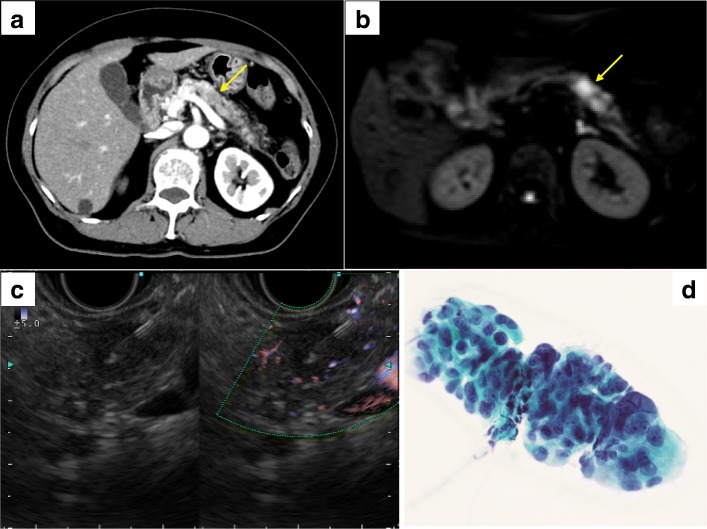
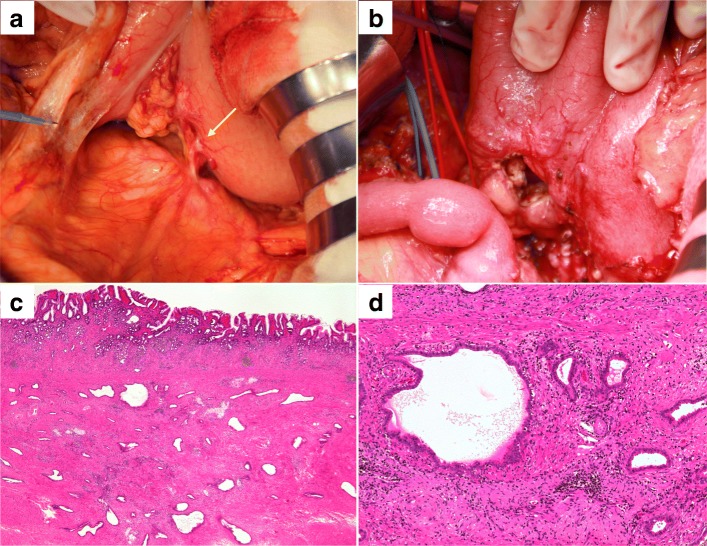
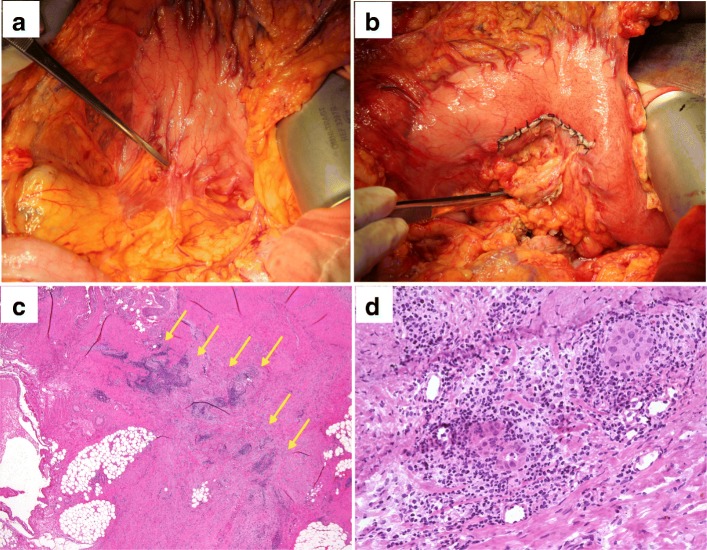
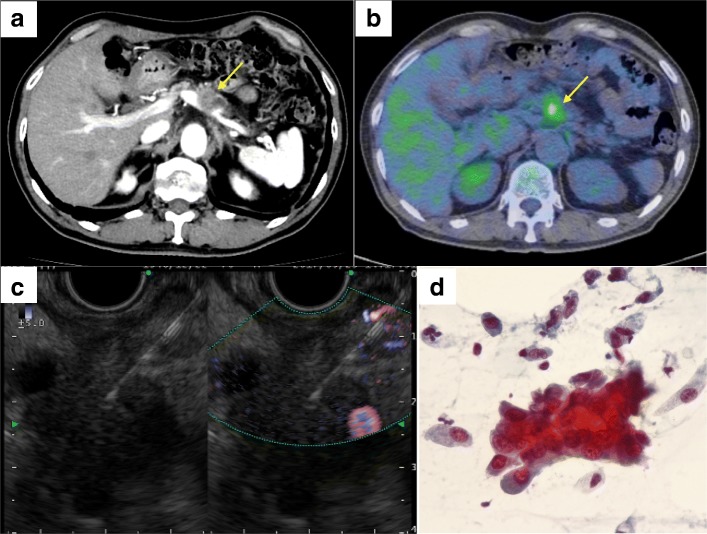
Case 1: A 68-year-old woman was admitted to our hospital for persistent cough. Computed tomography (CT) scan revealed inflammatory changes in the left lung field, and incidentally, a 15-mm hypovascular mass was detected in the pancreatic body. She underwent EUS-FNA and was diagnosed as pancreatic adenocarcinoma. She underwent distal pancreatectomy with splenectomy; however, a small hard mass was observed in the posterior gastric wall during surgery. We performed partial gastrectomy, and the resected specimen was diagnosed as a needle tract seeding following EUS-FNA. She then underwent adjuvant chemotherapy with TS-1, but the pancreatic cancer showed recurrence 6 months after surgery. She died due to peritoneal dissemination 18 months after surgery. Case 2: A 70-year-old man was incidentally detected with a pancreatic body mass on a CT scan as part of his follow-up for recurrence of basal cell carcinoma. He underwent EUS-FNA and was diagnosed as pancreatic adenocarcinoma. He had nodules in both lungs, and it was difficult to differentiate them from lung metastasis of pancreatic cancer. Therefore, he underwent neoadjuvant chemoradiotherapy, and thereafter, the lung nodules showed no changes; hence, he underwent distal pancreatectomy with splenectomy. During surgery, we observed a hard mass in the posterior gastric wall. We performed partial gastrectomy, and the resected specimen was diagnosed as needle tract seeding due to EUS-FNA. He underwent chemotherapy with TS-1, and he is still alive 18 months after surgery at the time of writing.
For resectable pancreatic body or tail tumors, EUS-FNA should be carefully performed to prevent needle tract seeding and intraoperative as well as postoperative assessment for gastric wall metastasis is mandatory.
内镜超声引导下细针抽吸术(EUS-FNA)是诊断胰腺癌的有用工具。然而,该操作本身可能导致腹膜扩散和穿刺部位的针道种植。本文报告了 2 例 EUS-FNA 后因针道种植导致胃壁转移的病例。
病例 1:一名 68 岁女性因持续性咳嗽入住我院。计算机断层扫描(CT)显示左肺野炎症性改变,偶然发现胰体部有 15mm 低血管肿块。行 EUS-FNA 检查,诊断为胰腺腺癌。行胰体尾切除术加脾切除术;然而,术中发现胃后壁有一小硬肿块。我们行部分胃切除术,切除标本诊断为 EUS-FNA 后的针道种植。术后给予替吉奥化疗,但术后 6 个月胰腺癌复发。术后 18 个月死于腹膜扩散。病例 2:一名 70 岁男性在 CT 扫描中偶然发现胰体部肿块,这是基底细胞癌复发的随访检查。行 EUS-FNA 检查,诊断为胰腺腺癌。双肺有结节,难以与胰腺癌肺转移相鉴别。因此,行新辅助放化疗,此后肺部结节无变化,行胰体尾加脾切除术。术中发现胃后壁有硬肿块。行部分胃切除术,切除标本诊断为 EUS-FNA 后的针道种植。给予替吉奥化疗,截至写稿时,术后 18 个月仍存活。
对于可切除的胰体或胰尾部肿瘤,EUS-FNA 应谨慎操作,以防止针道种植,并需进行术中及术后胃壁转移的评估。