Batsis John A, Gilbert-Diamond Diane, McClure Auden C, Weintraub Aaron, Sette Diane, Mecchella John N, Rotenberg Sivan, Cook Summer B, Rothstein Richard I
Geisel School of Medicine at Dartmouth, Hanover, NH, USA.
Department of Medicine, Dartmouth-Hitchcock Medical Center, Lebanon, NH, USA.
Clin Med Insights Arthritis Musculoskelet Disord. 2019 Jul 23;12:1179544119862288. doi: 10.1177/1179544119862288. eCollection 2019.
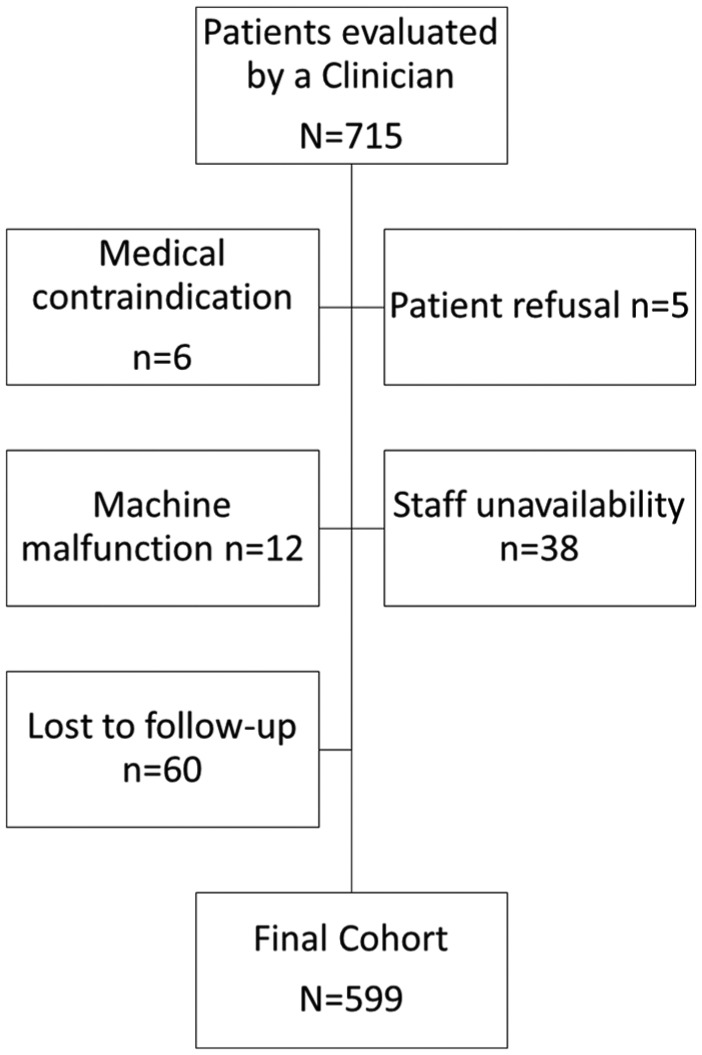
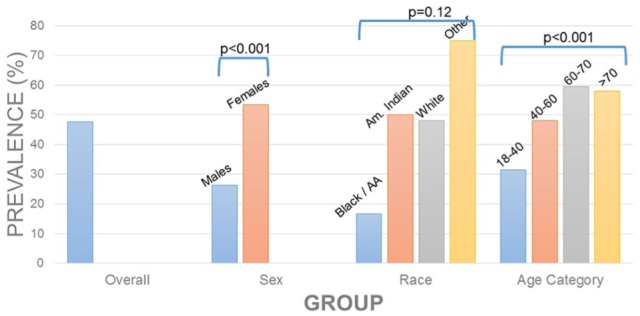
Sarcopenic obesity portends poor outcomes, yet it is under-recognized in practice. We collected baseline clinical data including data on body composition (total and segmental muscle mass and total body fat), grip strength, and 5-times sit-to-stand. We defined sarcopenia using cut-points for appendicular lean mass (ALM) and obesity using body-fat cut-points. A total of 599 clinic patients (78.5% female; mean age was 51.3 ± 14.2 years) had bioelectrical impedance analysis (BIA) data (83.8%). Mean body mass index (BMI) and waist circumference were 43.1 ± 8.9 kg/m and 132.3 ± 70.7 cm, respectively. All patients had elevated body fat. There were 284 (47.4%) individuals fulfilling criteria for ALM-defined sarcopenia. Sarcopenic obese persons had a lower BMI (38.2 ± 6.4 vs 47.6 ± 8.6; < 0.001), fat-free mass (113.0 kg ± 16.1 vs 152.1 kg ± 29.4; < 0.001), fat mass (48.4% ± 5.9 vs 49.5% ± 6.2; = 0.03), and visceral adipose tissue (216.8 ± 106.3 vs 242.7 ± 133.6 cm; = 0.009) than those without sarcopenic obesity. Grip strength was lower in those with sarcopenic obesity (25.1 ± 8.0 vs 30.5 ± 11.3 kg; < 0.001) and sit-to-stand times were longer (12.4 ± 4.4 vs 10.8 second ± 4.6; = 0.03). Sarcopenic obesity was highly prevalent in a rural, tertiary care weight and wellness center.
肌少性肥胖预示着不良后果,但在实际中却未得到充分认识。我们收集了基线临床数据,包括身体成分(全身和分段肌肉量以及全身脂肪)、握力和5次坐立试验的数据。我们使用四肢瘦体重(ALM)的切点来定义肌少症,使用体脂切点来定义肥胖。共有599名门诊患者(78.5%为女性;平均年龄为51.3±14.2岁)有生物电阻抗分析(BIA)数据(83.8%)。平均体重指数(BMI)和腰围分别为43.1±8.9kg/m²和132.3±70.7cm。所有患者的体脂均升高。有284名(47.4%)个体符合ALM定义的肌少症标准。与无肌少性肥胖的人相比,肌少性肥胖者的BMI较低(38.2±6.4 vs 47.6±8.6;P<0.001)、去脂体重较低(113.0kg±16.1 vs 152.1kg±29.4;P<0.001)、脂肪量较低(48.4%±5.9 vs 49.5%±6.2;P=0.03)以及内脏脂肪组织较低(216.8±106.3 vs 242.7±133.6cm;P=0.009)。肌少性肥胖者的握力较低(25.1±8.0 vs 30.5±11.3kg;P<0.001),坐立时间较长(12.4±4.4 vs 10.8秒±4.6;P=0.03)。在一家农村三级医疗体重与健康中心,肌少性肥胖非常普遍。