Arulkumaran Nish, Navaratnarajah Arunraj, Pillay Camilla, Brown Wendy, Duncan Neill, McLean Adam, Taube David, Brown Edwina A
Renal Section, Department of Medicine, Hammersmith Hospital Campus, Imperial College London, London, UK.
Clin Kidney J. 2018 Dec 22;12(4):550-558. doi: 10.1093/ckj/sfy118. eCollection 2019 Aug.
Patients who require acute initiation of dialysis have higher mortality rates when compared with patients with planned starts. Our primary objective was to explore the reasons and risk factors for acute initiation of renal replacement therapy (RRT) among patients with end-stage kidney disease (ESKD). Our secondary objective was to determine the difference in glomerular filtration rate (GFR) change in the year preceding RRT between elective and acute dialysis starts.
We conducted a single-centre retrospective observational study. ESKD patients either started dialysis electively (planned starters) or acutely and were known to renal services for >90 (unplanned starters) or <90 days (urgent starters).
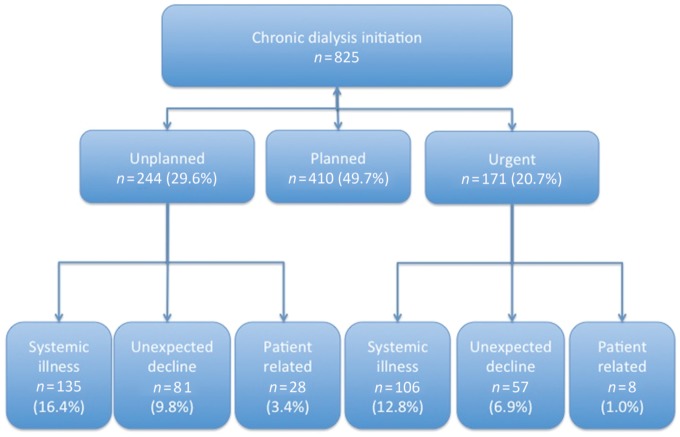
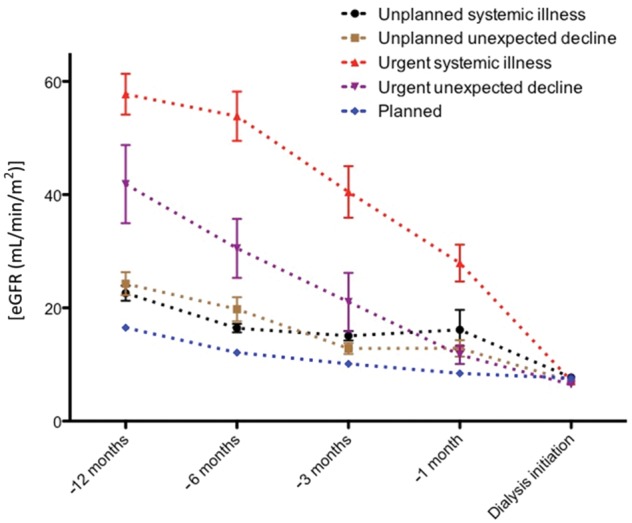
In all, 825 consecutive patients initiated dialysis between January 2013 and December 2015. Of these, 410 (49.7%) patients had a planned start. A total of 415 (50.3%) patients had an acute start on dialysis: 244 (58.8%) unplanned and 171 (41.2%) urgent. The reasons for acute dialysis initiation included acute illness (58%) and unexplained decline to ESKD (33%). Cardiovascular disease [ = 30 (22%)] and sepsis [ = 65 (48%)] accounted for the majority of acute systemic illness. Age and premorbid cardiovascular disease were independent risk factors for acute systemic illness among unplanned starts, whereas autoimmune disease accounted for the majority of urgent starts. The rate of decline in GFR was greater in the month preceding RRT among acute dialysis starters compared with planned starters (P < 0.001).
Cardiovascular disease and advancing age were independent risk factors for emergency dialysis initiation among patients known to renal services for >3 months. The rapid and often unpredictable loss of renal function in the context of acute systemic illness poses a challenge to averting emergency dialysis start.
与计划开始透析的患者相比,需要急性开始透析的患者死亡率更高。我们的主要目标是探讨终末期肾病(ESKD)患者急性开始肾脏替代治疗(RRT)的原因和危险因素。我们的次要目标是确定择期和急性透析开始的患者在RRT前一年肾小球滤过率(GFR)变化的差异。
我们进行了一项单中心回顾性观察研究。ESKD患者要么择期开始透析(计划开始者),要么急性开始透析,并且已知在肾脏服务机构就诊超过90天(非计划开始者)或少于90天(紧急开始者)。
2013年1月至2015年12月期间,共有825例连续患者开始透析。其中,410例(49.7%)患者为计划开始。共有415例(50.3%)患者急性开始透析:244例(58.8%)非计划开始,171例(41.2%)紧急开始。急性透析开始的原因包括急性疾病(58%)和原因不明的ESKD病情恶化(33%)。心血管疾病[=30例(22%)]和脓毒症[=65例(48%)]占急性全身性疾病的大多数。年龄和病前心血管疾病是非计划开始透析患者急性全身性疾病的独立危险因素,而自身免疫性疾病占紧急开始透析患者的大多数。与计划开始透析的患者相比,急性透析开始的患者在RRT前一个月GFR下降速度更快(P<0.001)。
对于在肾脏服务机构就诊超过3个月的患者,心血管疾病和年龄增长是紧急透析开始的独立危险因素。在急性全身性疾病背景下,肾功能快速且往往不可预测的丧失对避免紧急透析开始构成挑战。