Department of Urology, Nara Medical University, Nara, Japan.
Department of Psychiatry, Nara Medical University, Nara, Japan.
Cancer Sci. 2019 Oct;110(10):3315-3327. doi: 10.1111/cas.14158. Epub 2019 Aug 19.
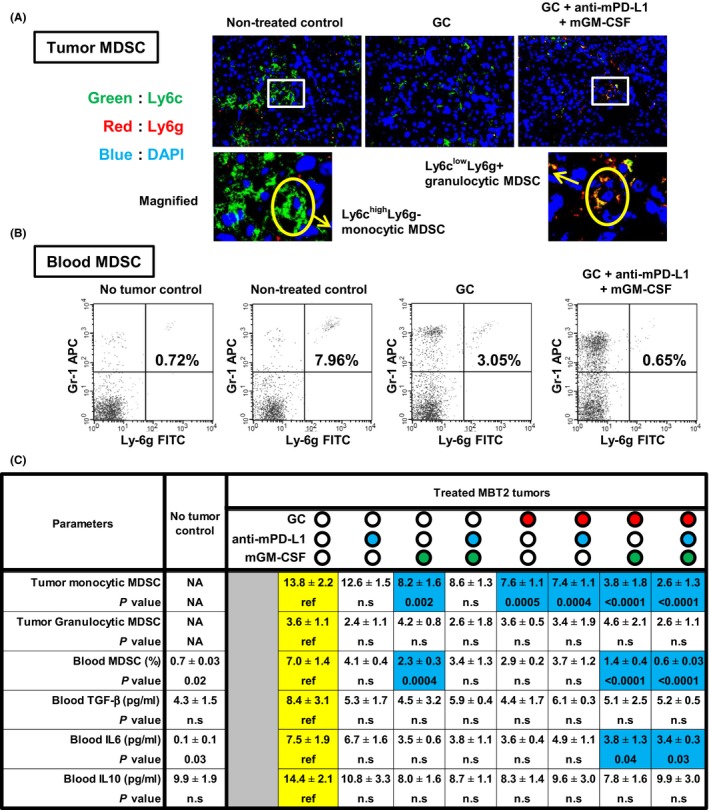
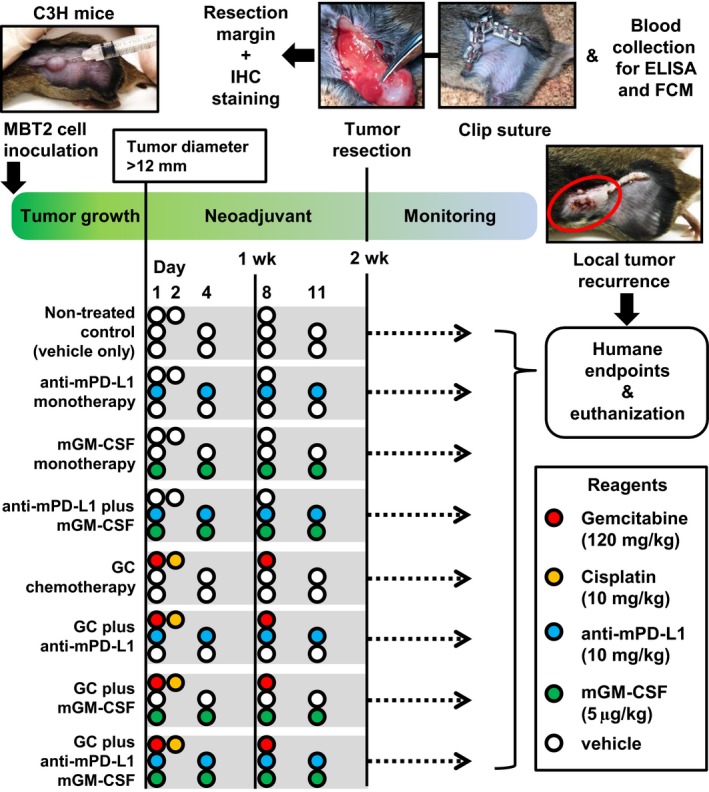
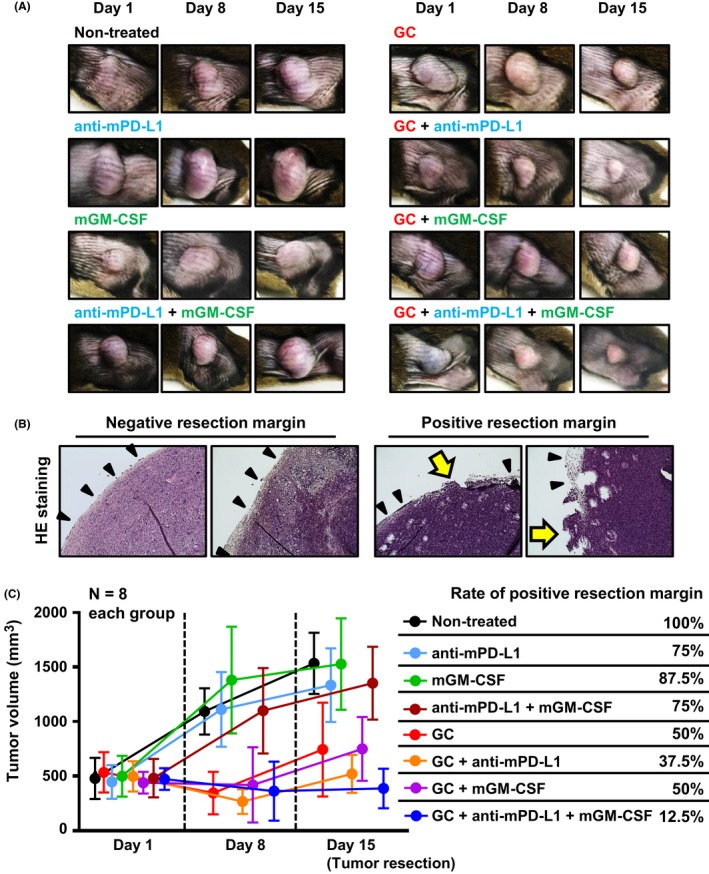
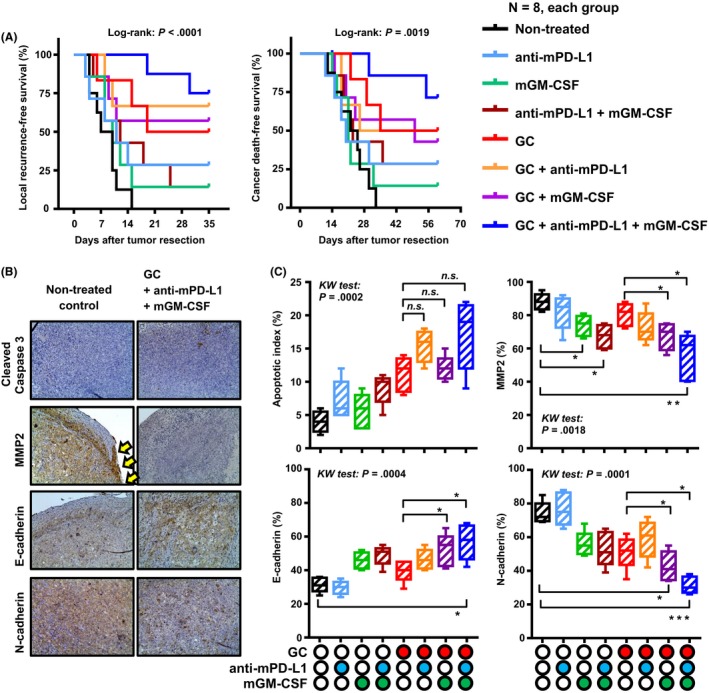
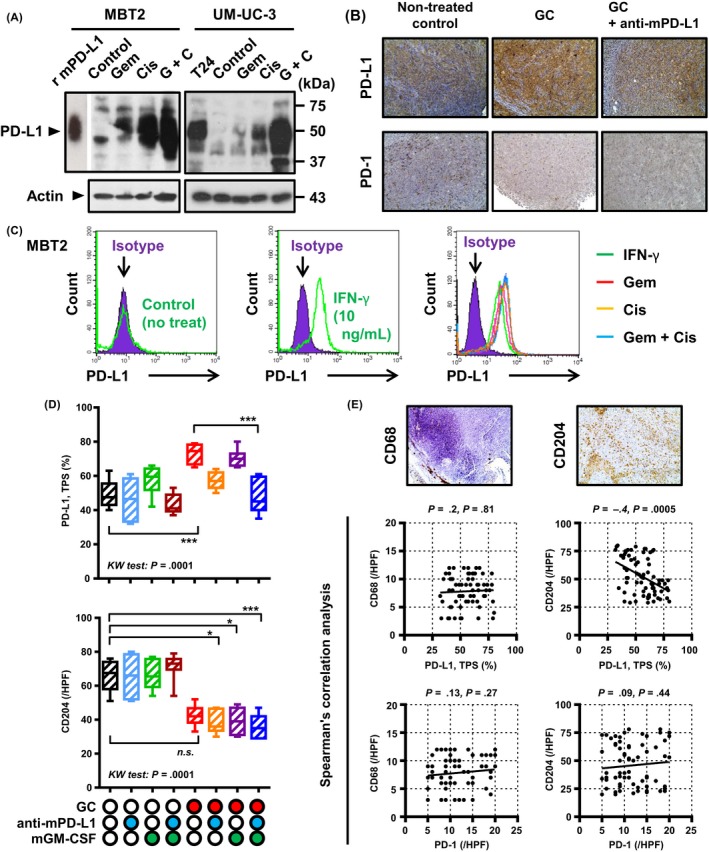
Despite advances and refinements in surgery and perioperative chemotherapy, there are still unmet medical needs with respect to radical cystectomy for muscle-invasive bladder cancer (MIBC). We investigated the potential benefit of supplementary granulocyte macrophage colony-stimulating factor (GM-CSF) to chemoimmunotherapy with programmed cell death protein-1 (PD-1)/programmed death-ligand 1 (PD-L1) axis blockade and standard neoadjuvant chemotherapy in bladder cancer. We inoculated 2 × 10 MBT2 cells s.c. in C3H mice to create a syngeneic animal model of local recurrence (LR). When the tumor diameter reached 12 mm, the mice were allocated randomly as follows: (i) non-treated control (vehicle only); (ii) anti-mPD-L1 monotherapy; (iii) mGM-CSF monotherapy; (iv) anti-mPD-L1 plus mGM-CSF; (v) gemcitabine and cisplatin (GC); (vi) GC plus anti-mPD-L1; (vii) GC plus mGM-CSF; and (viii) GC plus anti-mPD-L1 plus mGM-CSF. After completing 2-week neoadjuvant therapy, tumors were resected for resection margin evaluation and immunohistochemical staining and blood was collected for flow cytometry and ELISA. Operative wounds were sutured, and the operative site was monitored to detect LR. Addition of anti-mPD-L1 and mGM-CSF to neoadjuvant GC chemotherapy enhanced the antitumor effect and reduced positive resection margins (50% vs 12.5%). Combination of GC, anti-mPD-L1, and mGM-CSF resulted in longer LR-free survival and cancer-specific survival compared to those in other groups. These effects involved an immunotherapy-related decrease in oncological properties such as tumor invasion capacity and epithelial-mesenchymal transition. mGM-CSF significantly decreased the accumulation of myeloid-derived suppressor cells in both the blood and tumor microenvironment and blood interleukin-6 levels. Supplementary GM-CSF to neoadjuvant GC plus PD-L1 blockade could decrease LR after radical surgery by immune modulation in the blood and tumor microenvironment.
尽管在手术和围手术期化疗方面取得了进展和改进,但对于肌层浸润性膀胱癌(MIBC)的根治性膀胱切除术,仍存在未满足的医疗需求。我们研究了补充粒细胞巨噬细胞集落刺激因子(GM-CSF)对 PD-1/PD-L1 轴阻断和标准新辅助化疗联合化疗免疫治疗在膀胱癌中的潜在益处。我们将 2×10 的 MBT2 细胞皮下接种到 C3H 小鼠中,以建立局部复发(LR)的同源动物模型。当肿瘤直径达到 12mm 时,将小鼠随机分配如下:(i)未治疗对照(仅给予载体);(ii)抗 mPD-L1 单药治疗;(iii)mGM-CSF 单药治疗;(iv)抗 mPD-L1 加 mGM-CSF;(v)吉西他滨和顺铂(GC);(vi)GC 加抗 mPD-L1;(vii)GC 加 mGM-CSF;和(viii)GC 加抗 mPD-L1 加 mGM-CSF。完成 2 周新辅助治疗后,切除肿瘤进行切缘评估和免疫组织化学染色,并采集血液进行流式细胞术和 ELISA 检测。缝合手术伤口,并监测手术部位以检测 LR。在新辅助 GC 化疗中加入抗 mPD-L1 和 mGM-CSF 可增强抗肿瘤作用并减少阳性切缘(50%对 12.5%)。与其他组相比,GC、抗 mPD-L1 和 mGM-CSF 的联合使用导致无 LR 生存和癌症特异性生存时间更长。这些作用涉及免疫治疗相关的降低肿瘤侵袭能力和上皮-间充质转化等肿瘤学特性。mGM-CSF 可显著减少骨髓来源的抑制细胞在血液和肿瘤微环境中的积累以及血液中白细胞介素-6 水平。新辅助 GC 加 PD-L1 阻断后补充 GM-CSF 可通过血液和肿瘤微环境中的免疫调节减少根治性手术后的 LR。