EA-3801, SFR CAP-santé, Université de Reims Champagne-Ardenne, 51092, Reims Cedex, France.
Laboratoire d'Hématologie, CHU Robert Debré, Reims, France.
J Transl Med. 2019 Aug 9;17(1):261. doi: 10.1186/s12967-019-2003-3.
Cell therapy has been proposed for patients with critical limb ischemia (CLI). Autologous bone marrow derived cells (BMCs) have been mostly used, mesenchymal stem cells (MSCs) being an alternative. The aim of this study was to characterize two types of MSCs and evaluate their efficacy.
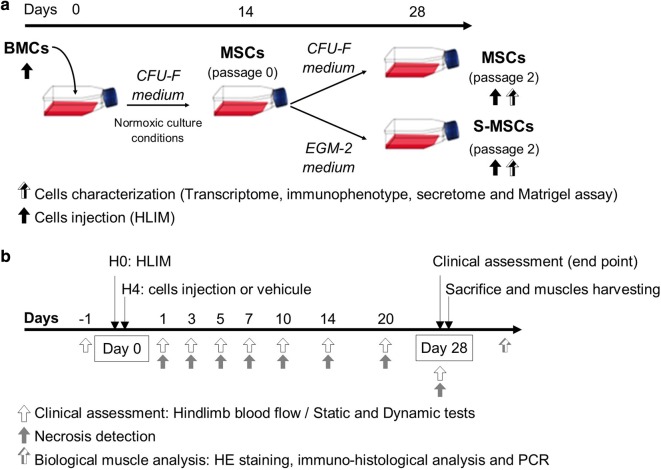
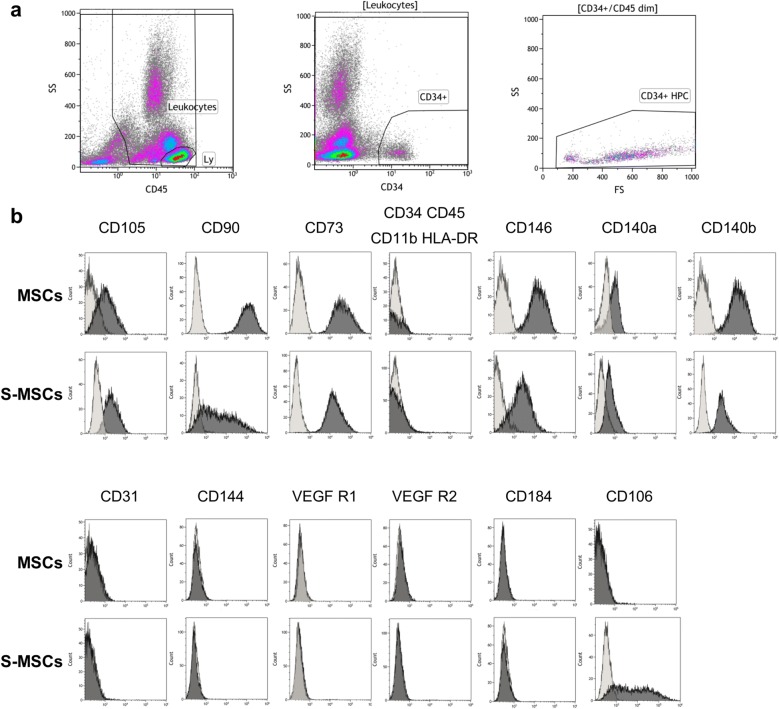
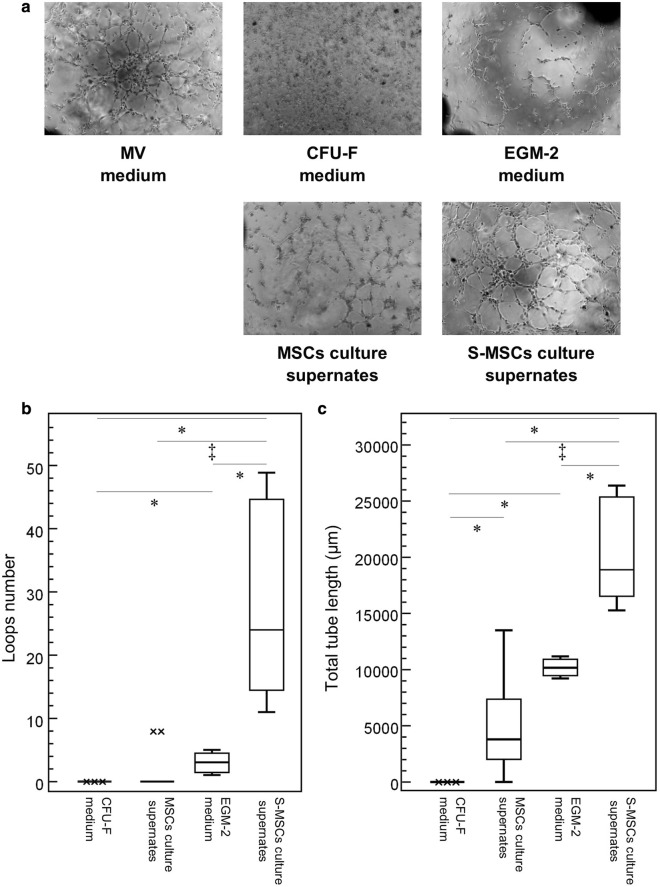
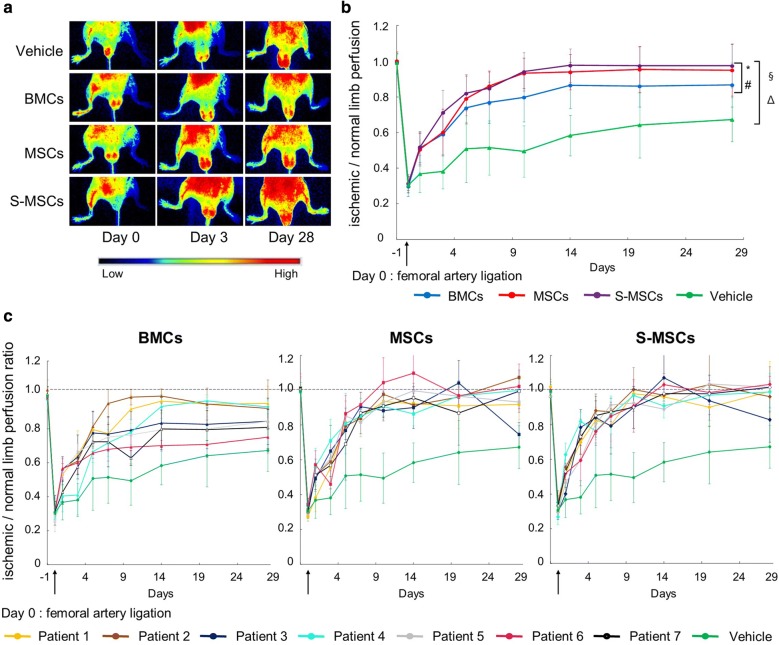
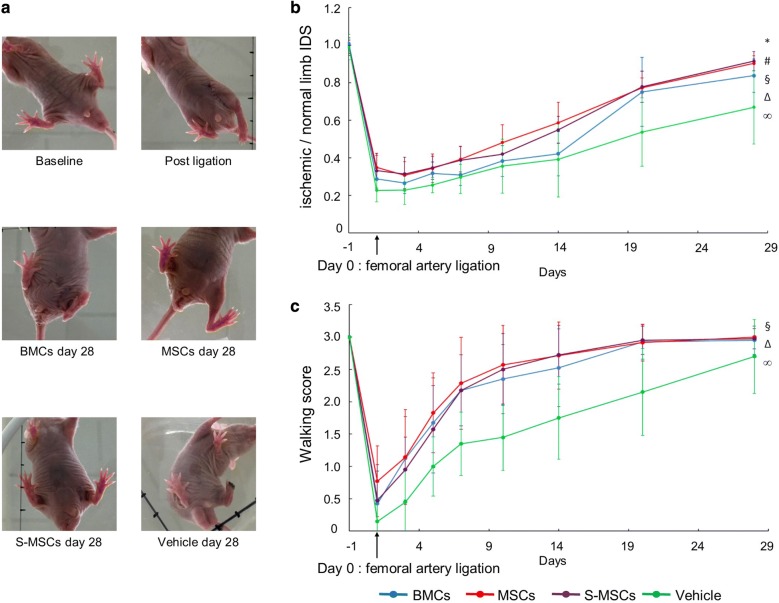
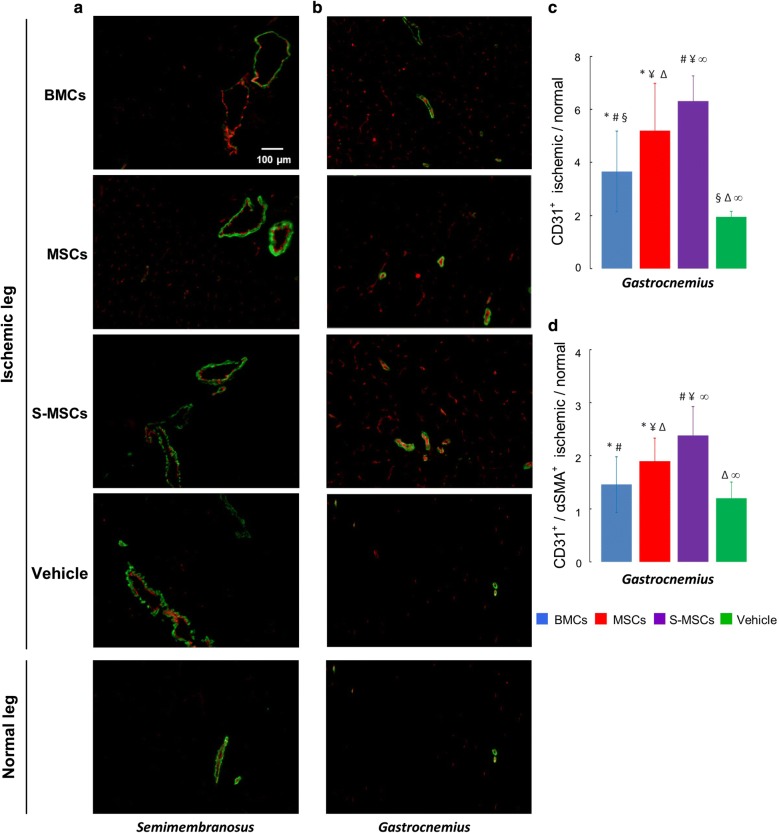
MSCs were obtained from CLI-patients BMCs. Stimulated- (S-) MSCs were cultured in endothelial growth medium. Cells were characterized by the expression of cell surface markers, the relative expression of 6 genes, the secretion of 10 cytokines and the ability to form vessel-like structures. The cell proangiogenic properties was analysed in vivo, in a hindlimb ischemia model. Perfusion of lower limbs and functional tests were assessed for 28 days after cell infusion. Muscle histological analysis (neoangiogenesis, arteriogenesis and muscle repair) was performed.
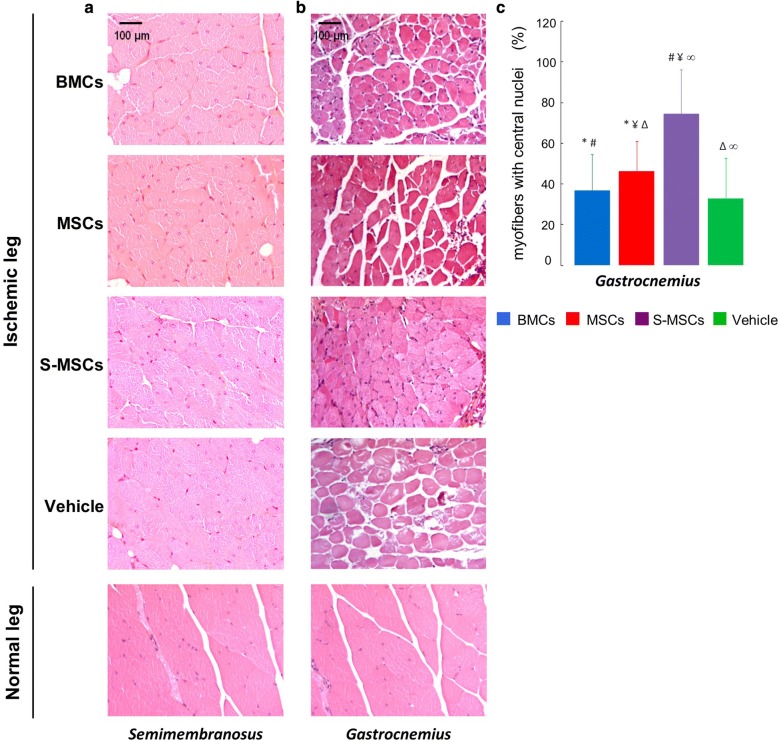
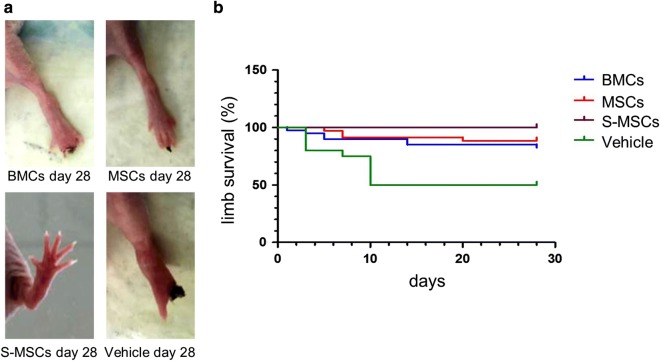
S-MSCs can be obtained from CLI-patients BMCs. They do not express endothelial specific markers but can be distinguished from MSCs by their secretome. S-MSCs have the ability to form tube-like structures and, in vivo, to induce blood flow recovery. No amputation was observed in S-MSCs treated mice. Functional tests showed improvement in treated groups with a superiority of MSCs and S-MSCs. In muscles, CD31+ and αSMA+ labelling were the highest in S-MSCs treated mice. S-MSCs induced the highest muscle repair.
S-MSCs exert angiogenic potential probably mediated by a paracrine mechanism. Their administration is associated with flow recovery, limb salvage and muscle repair. The secretome from S-MSCs or secretome-derived products may have a strong potential in vessel regeneration and muscle repair. Trial registration NCT00533104.
细胞疗法已被提议用于治疗严重肢体缺血(CLI)患者。自体骨髓来源的细胞(BMCs)已被广泛应用,间充质干细胞(MSCs)则是另一种选择。本研究旨在对两种类型的 MSCs 进行特征描述并评估其疗效。
从 CLI 患者的 BMC 中获取 MSCs。刺激的(S-)MSCs 在血管内皮生长培养基中培养。通过细胞表面标志物的表达、6 个基因的相对表达、10 种细胞因子的分泌以及形成管状结构的能力来对细胞进行特征描述。在一个后肢缺血模型中,对细胞的促血管生成特性进行体内分析。在细胞输注后 28 天评估下肢灌注和功能测试。进行肌肉组织学分析(新生血管形成、动脉生成和肌肉修复)。
可以从 CLI 患者的 BMC 中获得 S-MSCs。它们不表达内皮特异性标志物,但可以通过其分泌组与 MSCs 区分开来。S-MSCs 具有形成管状结构的能力,并能在体内诱导血流恢复。在接受 S-MSCs 治疗的小鼠中没有观察到截肢。功能测试显示治疗组有改善,其中 MSC 和 S-MSCs 具有优势。在肌肉中,S-MSCs 治疗的小鼠中 CD31+和αSMA+标记最高。S-MSCs 诱导的肌肉修复最高。
S-MSCs 通过旁分泌机制发挥血管生成潜能。它们的给药与血流恢复、肢体挽救和肌肉修复有关。S-MSCs 的分泌组或分泌组衍生产物可能具有很强的血管再生和肌肉修复潜力。试验注册号:NCT00533104。