Department of Medicine, Ruby Hall Clinic, Pune, Maharashtra, India.
Department of Medicine, Poona Hospital and Research Centre, Pune, Maharashtra, India.
BMC Infect Dis. 2019 Aug 13;19(1):714. doi: 10.1186/s12879-019-4361-0.
Despite rapid scale up of antiretroviral therapy (ART), Tuberculosis (TB) remains the commonest opportunistic infection and cause of death among HIV infected individuals in resource limited settings like India. Incidence of TB in individuals on ART in private healthcare sector in India is infrequently studied.
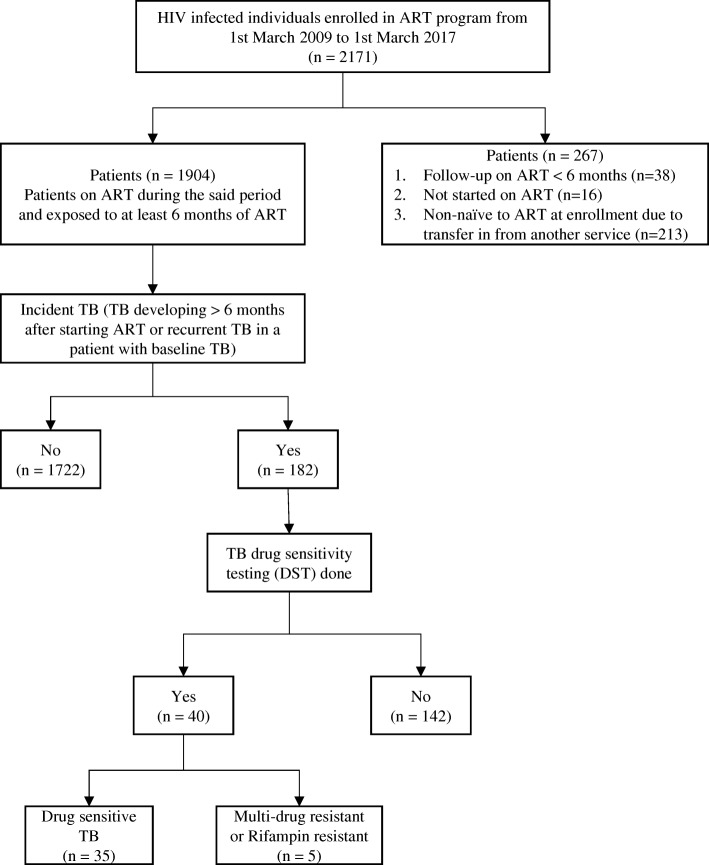
This retrospective cohort study conducted between 1st March 2009 and 1st March 2017 aimed to evaluate rate of incident TB in individuals initiated on ART at 3 private sector ART clinics in Pune, India. Individuals more than 12 years of age with ART duration of atleast 6 months were included. Patients were classified as having prevalent TB if they had a TB episode within the year prior to ART initiation or if they developed TB within 6 months of starting ART. Individuals who were diagnosed with TB after 6 months of starting ART were classified as incident TB cases. A recurrent episode of TB after treatment completion or cure of prevalent TB was also regarded as incident TB. Patients were classified as definitive TB if Mycobacterium tuberculosis was grown in culture from a biological sample or a positive rapid molecular test. Patients were classified as probable TB if there was radiologic evidence of TB in absence of confirmatory culture or PCR.
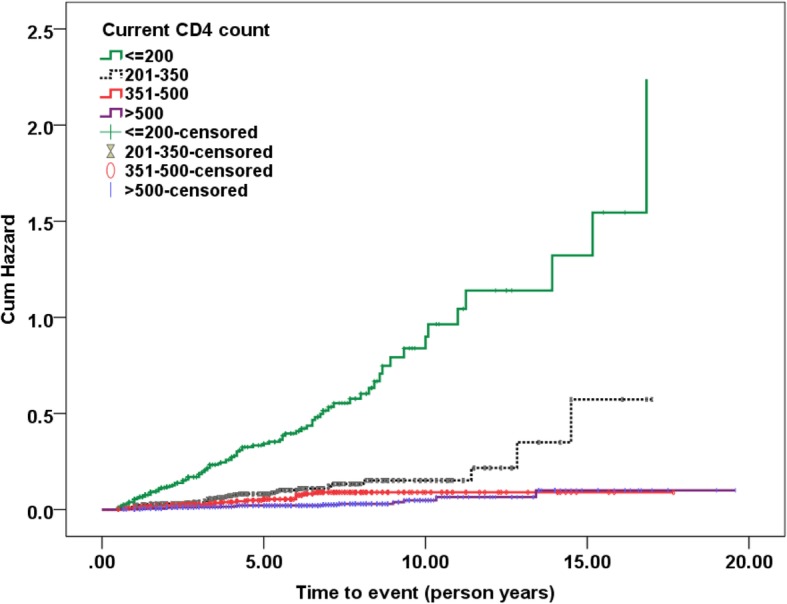
1904 patients with a median duration of follow up on ART of 57 (IQR = 32.0, 84.0) months were included. Of these, 182 developed incident TB (22% definitive TB, 38% recurrent cases). TB incidence at 6-12 months, 13-24 months, 25-60 months and > 60 months of ART was 24.32, 5.46, 2.54 and 0.75 cases per 100 person years respectively. Current time updated CD4 count < 500 cells/mm (p < 0.0001), virologic failure on ART (adjusted Hazard Ratio (aHR): 3.05 (95% CI: 2.094, 4.454), p < 0.0001) and receipt of ART without IPT (aHR: 8.24 (95% CI, 3.358, 20.204), p < 0.0001) were associated with higher risk of incident TB.
Starting ART early in treatment naïve individuals, prompt detection of virologic failure on ART and providing IPT along with ART will be useful in reducing incident TB. Efforts from private sector are crucial in achieving Sustainable Development Goals set by Government of India and attaining the vision of a TB free India.
尽管抗逆转录病毒疗法(ART)迅速推广,但在资源有限的环境中,如印度,结核病仍然是艾滋病毒感染者中最常见的机会性感染和死亡原因。在印度私营医疗保健部门,接受 ART 治疗的个体中结核病的发病率很少被研究。
这项回顾性队列研究于 2009 年 3 月 1 日至 2017 年 3 月 1 日在印度浦那的 3 家私营部门 ART 诊所进行,旨在评估在这些诊所开始接受 ART 的个体中结核病的发病率。年龄在 12 岁以上,ART 持续时间至少 6 个月的个体被纳入研究。如果个体在开始 ART 前一年有过结核病发作,或者在开始 ART 后 6 个月内出现结核病,则将其归类为现患结核病。如果个体在开始 ART 后 6 个月后被诊断出结核病,则将其归类为新发结核病病例。在完成治疗或治愈现患结核病后再次出现结核病也被视为新发结核病。如果从生物样本中培养出结核分枝杆菌或快速分子检测呈阳性,则将个体归类为确诊结核病。如果没有确认性培养或 PCR,但有结核病的影像学证据,则将个体归类为可能结核病。
共有 1904 名接受 ART 治疗的个体纳入研究,中位 ART 治疗随访时间为 57(IQR=32.0,84.0)个月。其中 182 名个体发生了新发结核病(22%为确诊结核病,38%为复发病例)。在 ART 治疗的 6-12 个月、13-24 个月、25-60 个月和>60 个月时,结核病发病率分别为每 100 人年 24.32、5.46、2.54 和 0.75 例。目前更新的 CD4 计数<500 个细胞/mm(p<0.0001)、ART 治疗病毒学失败(调整后的危险比[aHR]:3.05(95%CI:2.094,4.454),p<0.0001)和未接受 IPT 的 ART 治疗(aHR:8.24(95%CI,3.358,20.204),p<0.0001)与新发结核病的风险增加相关。
在治疗初治个体时尽早开始 ART,及时发现 ART 病毒学失败,并在 ART 治疗的同时提供 IPT,将有助于降低新发结核病的发病率。私营部门的努力对于实现印度政府制定的可持续发展目标和实现印度无结核病的愿景至关重要。