Mekelle University College of Health Sciences, Mekelle, Ethiopia.
Hayat General Hospital, Addis Ababa, Ethiopia.
PLoS One. 2020 May 22;15(5):e0233049. doi: 10.1371/journal.pone.0233049. eCollection 2020.
The role of CD4/CD8 ratio on the incidence of tuberculosis (TB) in patients on antiretroviral therapy (ART) is unknown. Thus, we sought to determine whether the CD4/CD8 ratio was associated with development of TB in a cohort of HIV infected individuals on ART followed up for more than a decade in the setting of sub-Saharan Africa (SSA).
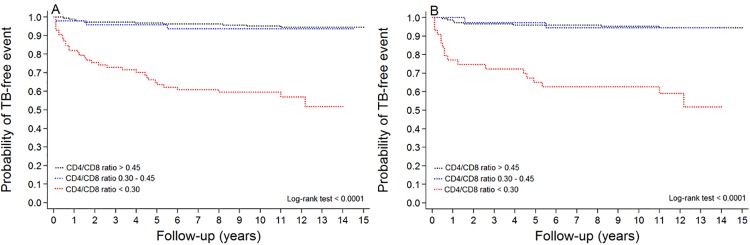
The cohort comprised adult patients who started ART between 2001 and 2007 and followed for up to 15 years. Clinical data were collected in retrospective manner. Patients with an AIDS defining illness or a CD4 count <200 cell/μL were started with a combination of ART. The participants have clinic visits every 6 months and/or as needed. Poisson regression models were used to identify factors associated with development of incident TB. Kaplan-Meier curves were used to estimate the probability of incident TB while on ART.
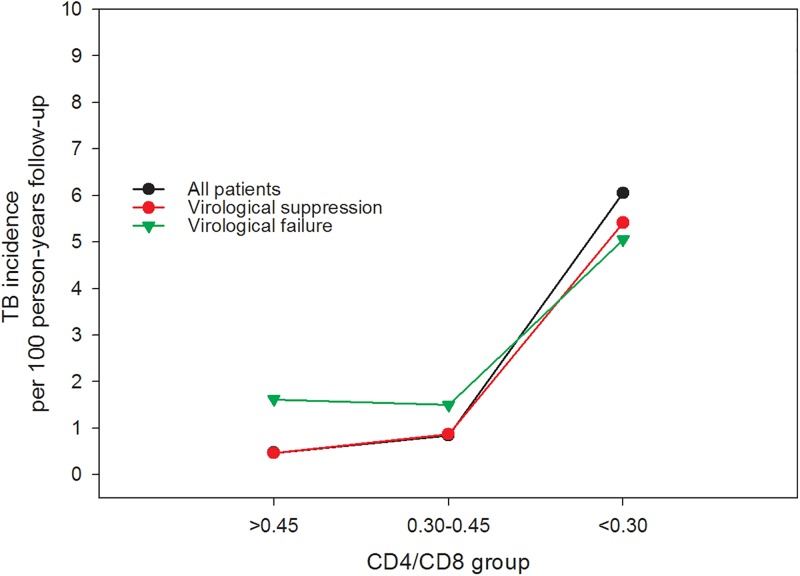
A total of 347 patients with a median duration of follow-up on ART of 11.5 (IQR: 10.0-12.5) years were included. Incident TB developed in 47 patients during the 3259 person-years of follow-up, the majority (76.6%) occurred within five year of ART initiation. On univariate analysis, poor ART adherence (RR:2.57, 95% CI: 1.28-5.17), time-updated CD4 cell count of lower than 200 (RR: 4.86, 95%CI 2.33-10.15), or CD4 cell count between 200 and 500 (RR: 4.68, 95% CI: 2.17-10.09), time-updated CD8 cell count lower than 500 (RR: 2.83 95% CI 1.31-6.10), or CD8 cell count over 1000 (RR: 2.23, 95% CI: 1.12-4.45), time-updated CD4/CD8 ratio of less than 0.30 (RR: 6.00, 95% CI: 2.96-12.14), lack of normalization of CD4 T-cell count (RR: 6.13, 95% CI: 2.20-17.07), and virological failure (RR: 2.35 (95% CI: 1.17-4.71) were all associated with increased risk of incident TB. In multivariate analysis, however, time-updated CD4/CD8 ratio of less than 0.30 (adjusted RR: 4.08, 95% CI: 1.31-12.68) was the only factor associated with increased risk of developing incident TB (p = 0.015). Similar results were obtained in a sensitivity analysis by including only those virally suppressed patients (n = 233, 69% of all patients). In this group, CD4/CD8 ratio of less than 0.30 was associated with development of incident TB (adjusted RR: 4.02, 95% CI: 1.14-14.19, p = 0.031). Overall, the incidence rate of TB in patients with an updated CD4/CD8 ratio of less than 0.30 was more than 5-fold higher when compared with those with a ratio more than 0.45.
Low CD4/CD8 ratio is independently associated with an increased risk of incident TB despite viral suppression. CD4/CD8 ratio may serve as a biomarker for identifying patients at risk of TB in patients on ART in the setting of SSA.
CD4/CD8 比值在接受抗逆转录病毒治疗 (ART) 的艾滋病患者中发生结核病 (TB) 的作用尚不清楚。因此,我们试图确定在撒哈拉以南非洲 (SSA) 地区接受超过 10 年随访的 HIV 感染患者中,CD4/CD8 比值是否与 TB 的发生有关。
该队列包括在 2001 年至 2007 年间开始接受 ART 的成年患者,并随访了长达 15 年。以回顾性方式收集临床数据。有 AIDS 定义性疾病或 CD4 计数 <200 个/μL 的患者开始接受 ART 联合治疗。参与者每 6 个月或根据需要进行就诊。使用泊松回归模型确定与发生 TB 相关的因素。使用 Kaplan-Meier 曲线估计在 ART 期间发生 TB 的概率。
共纳入了 347 名中位 ART 随访时间为 11.5 年(IQR:10.0-12.5)的患者。在 3259 人年的随访中,47 名患者发生了 TB,其中大多数(76.6%)发生在 ART 开始后的五年内。在单变量分析中,ART 依从性差(RR:2.57,95%CI:1.28-5.17)、时间更新的 CD4 细胞计数低于 200(RR:4.86,95%CI 2.33-10.15)或 CD4 细胞计数在 200 至 500 之间(RR:4.68,95%CI 2.17-10.09)、时间更新的 CD8 细胞计数低于 500(RR:2.83 95%CI 1.31-6.10)或 CD8 细胞计数超过 1000(RR:2.23,95%CI 1.12-4.45)、时间更新的 CD4/CD8 比值小于 0.30(RR:6.00,95%CI 2.96-12.14)、CD4 T 细胞计数未恢复正常(RR:6.13,95%CI 2.20-17.07)和病毒学失败(RR:2.35(95%CI:1.17-4.71)均与发生 TB 的风险增加相关。然而,在多变量分析中,时间更新的 CD4/CD8 比值小于 0.30(调整后的 RR:4.08,95%CI:1.31-12.68)是唯一与发生 TB 的风险增加相关的因素(p = 0.015)。在仅包括病毒抑制患者的敏感性分析中(n = 233,所有患者的 69%)得到了类似的结果。在该组中,CD4/CD8 比值小于 0.30 与发生 TB 相关(调整后的 RR:4.02,95%CI:1.14-14.19,p = 0.031)。总体而言,与 CD4/CD8 比值大于 0.45 的患者相比,比值小于 0.30 的患者发生 TB 的发病率要高 5 倍以上。
尽管病毒得到抑制,但低 CD4/CD8 比值与发生 TB 的风险增加独立相关。CD4/CD8 比值可能是识别 SSA 地区接受 ART 治疗的患者中发生 TB 风险的生物标志物。