Section of Environment and Radiation, International Agency for Research on Cancer (IARC), 150 Cours Albert Thomas, Lyon, France.
Fred Hutchinson Cancer Research Center, Seattle, WA, USA.
Breast Cancer Res. 2019 Aug 13;21(1):93. doi: 10.1186/s13058-019-1174-4.
Improving breast cancer survival in sub-Saharan Africa (SSA) is urgently needed, requiring early diagnosis and improved access to treatment. However, data on the types of and barriers to receiving breast cancer therapy in this region are limited and have not been compared between different SSA countries and treatment settings.
In different health care settings across Uganda, Nigeria and Namibian sites of the prospective African Breast Cancer - Disparities in Outcomes cohort study, we assessed the percentage of newly diagnosed breast cancer patients who received treatment (systemic, surgery and/or radiotherapy) for cancer and their socio-demographic and clinical determinants. Treatment data were systematically extracted from medical records, as well as self-reported by women during 6-month follow-up interviews, and were used to generate a binary indicator of treatment received within 12 months of diagnosis (yes/no), which was analysed via logistic regression.
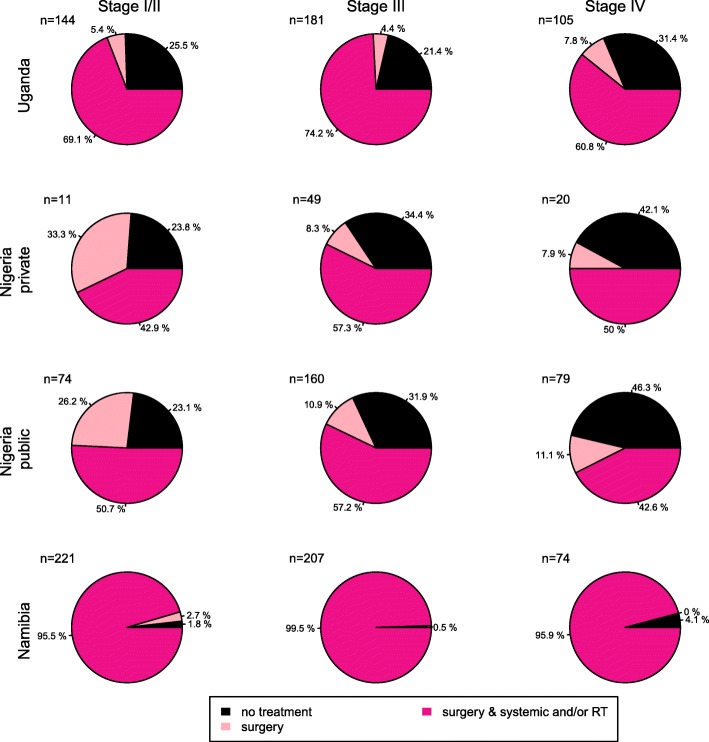
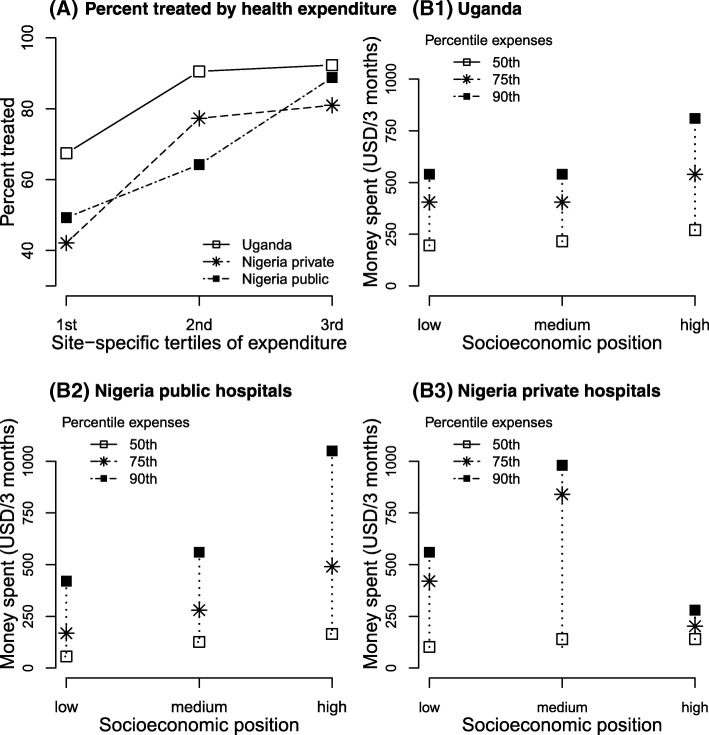
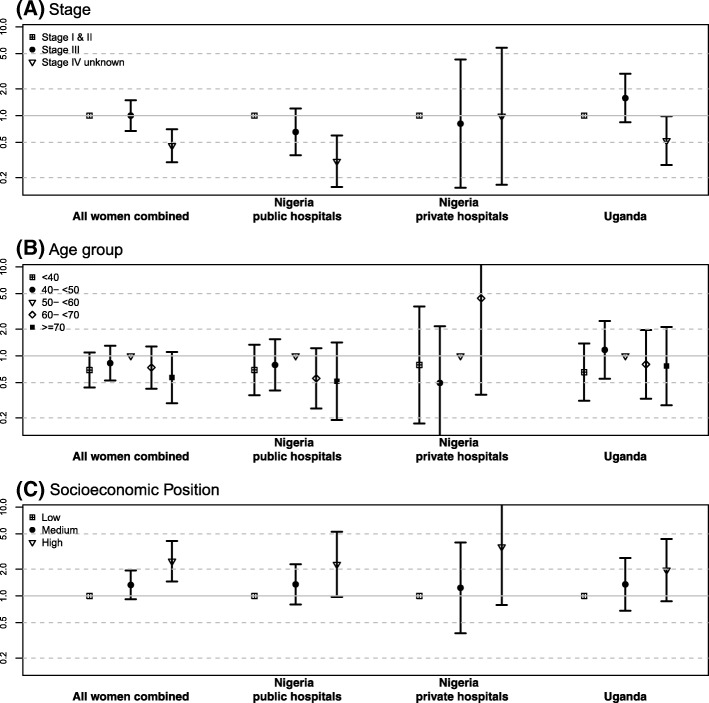
Of 1325 women, cancer treatment had not been initiated treatment within 1 year of diagnosis for 227 (17%) women and 185 (14%) of women with stage I-III disease. Untreated percentages were highest in two Nigerian regional hospitals where 38% of 314 women were not treated (32% among stage I-III). At a national referral hospital in Uganda, 18% of 430 women were not treated (15% among stage I-III). In contrast, at a cancer care centre in Windhoek, Namibia, where treatment is provided free to the patient, all non-black (100%) and almost all (98.7%) black women had initiated treatment. Percentages of untreated women were higher in women from lower socio-economic groups, women who believed in traditional medicine and, in Uganda, in HIV+ women. Self-reported treatment barriers confirmed treatment costs and treatment refusal as contributors to not receiving treatment.
Financial support to ensure treatment access and education of treatment benefits are needed to improve treatment access for breast cancer patients across sub-Saharan Africa, especially at regional treatment centres, for lower socio-economic groups, and for the HIV-positive woman with breast cancer.
迫切需要提高撒哈拉以南非洲(SSA)的乳腺癌生存率,这需要早期诊断和改善治疗机会。然而,关于该地区接受乳腺癌治疗的类型和障碍的数据有限,并且尚未在不同的 SSA 国家和治疗环境之间进行比较。
在乌干达、尼日利亚和纳米比亚的前瞻性非洲乳腺癌-结局差异队列研究的不同医疗保健环境中,我们评估了新诊断的乳腺癌患者中有多少人接受了癌症治疗(全身性、手术和/或放疗),并评估了他们的社会人口统计学和临床决定因素。治疗数据是从病历中系统提取的,也由女性在 6 个月随访访谈中自我报告,用于生成 12 个月内诊断后接受治疗的二进制指标(是/否),并通过逻辑回归进行分析。
在 1325 名女性中,有 227 名(17%)和 185 名(14%)患有 I-III 期疾病的女性在诊断后 1 年内未开始治疗。在两家尼日利亚地区医院中,未接受治疗的百分比最高,其中 314 名女性中有 38%未接受治疗(I-III 期患者中有 32%)。在乌干达的一家国家转诊医院中,有 430 名女性中有 18%未接受治疗(I-III 期患者中有 15%)。相比之下,在纳米比亚温得和克的癌症治疗中心,向患者免费提供治疗,所有非黑人(100%)和几乎所有(98.7%)黑人女性都开始了治疗。来自社会经济地位较低群体的女性、相信传统医学的女性以及乌干达的 HIV+女性中,未接受治疗的女性比例较高。自我报告的治疗障碍证实,治疗费用和治疗拒绝是导致未接受治疗的原因。
需要提供财政支持以确保获得治疗,并对治疗的益处进行教育,以改善撒哈拉以南非洲各地乳腺癌患者的治疗机会,特别是在地区治疗中心、社会经济地位较低的群体以及患有乳腺癌的 HIV+女性。