Ferrer Miquel, Sequeira Telma, Cilloniz Catia, Dominedo Cristina, Bassi Gianluigi Li, Martin-Loeches Ignacio, Torres Antoni
Department of Pneumology, Hospital Clinic of Barcelona, August Pi i Sunyer Biomedical Research Institute - IDIBAPS, University of Barcelona, 08036 Barcelona, Spain.
Network Centre for Biomedical Research in Respiratory Diseases (CibeRes, CB06/06/0028), Carlos III Health Institute, 28029 Madrid, Spain.
J Clin Med. 2019 Aug 14;8(8):1217. doi: 10.3390/jcm8081217.
Ventilator-associated pneumonia (VAP) is associated to longer stay and poor outcomes. Lacking definitive diagnostic criteria, worsening gas exchange assessed by PaO/FO ≤ 240 in mmHg has been proposed as one of the diagnostic criteria for VAP. We aim to assess the adequacy of PaO/FO ≤ 240 to diagnose VAP.
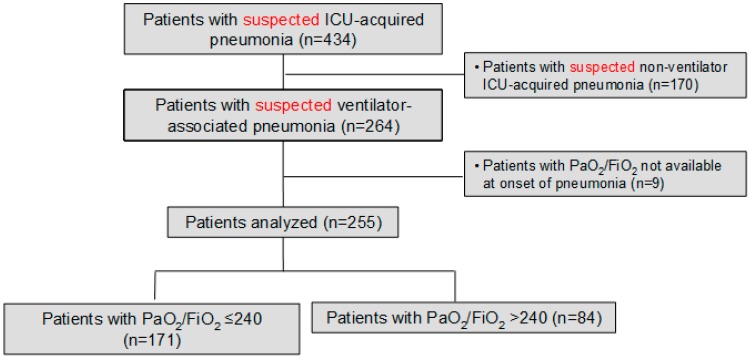
Prospective observational study in 255 consecutive patients with suspected VAP, clustered according to PaO/FO ≤ 240 vs. > 240 at pneumonia onset. The primary analysis was the association between PaO/FO ≤ 240 and quantitative microbiologic confirmation of pneumonia, the most reliable diagnostic gold-standard.
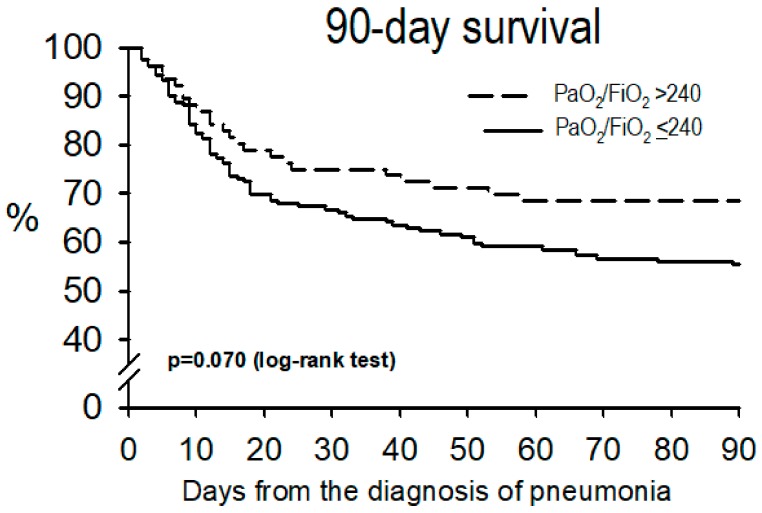
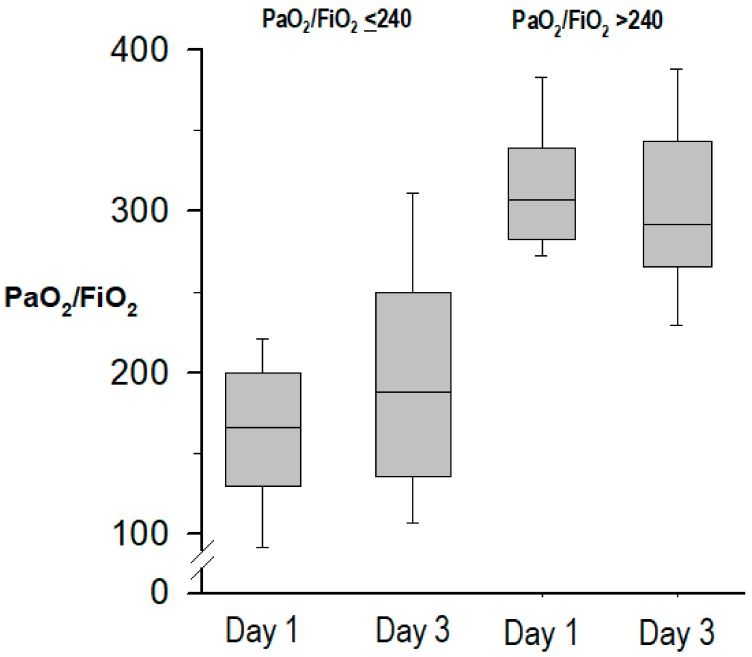
Mean PaO/FO at VAP onset was 195 ± 82; 171 (67%) cases had PaO/FO ≤ 240. Patients with PaO/FO ≤ 240 had a lower APACHE-II score at ICU admission; however, at pneumonia onset they had higher CPIS, SOFA score, acute respiratory distress syndrome criteria and incidence of shock, and less microbiological confirmation of pneumonia (117, 69% vs. 71, 85%, p = 0.008), compared to patients with PaO/FIO > 240. In multivariate logistic regression, PaO/FIO ≤ 240 was independently associated with less microbiological confirmation (adjusted odds-ratio 0.37, 95% confidence interval 0.15-0.89, = 0.027). The association between PaO/FO and microbiological confirmation of VAP was poor, with an area under the ROC curve 0.645. Initial non-response to treatment and length of stay were similar between both groups, while hospital mortality was higher in patients with PaO/FO ≤ 240.
Adding PaO/FO ratio ≤ 240 to the clinical and radiographic criteria does not help in the diagnosis of VAP. PaO/FO ratio > 240 does not exclude this infection. Using this threshold may underestimate the incidence of VAP.
呼吸机相关性肺炎(VAP)与住院时间延长及不良预后相关。由于缺乏明确的诊断标准,有人提出将动脉血氧分压/吸入氧分数(PaO₂/FiO₂)≤240 mmHg(毫米汞柱)时气体交换恶化作为VAP的诊断标准之一。我们旨在评估PaO₂/FiO₂≤240用于诊断VAP的适用性。
对255例连续疑似VAP患者进行前瞻性观察研究,根据肺炎发作时PaO₂/FiO₂≤240与>240进行分组。主要分析是PaO₂/FiO₂≤240与肺炎定量微生物学确诊之间的关联,肺炎定量微生物学确诊是最可靠的诊断金标准。
VAP发作时的平均PaO₂/FiO₂为195±82;171例(67%)患者的PaO₂/FiO₂≤240。PaO₂/FiO₂≤240的患者在重症监护病房(ICU)入院时急性生理与慢性健康状况评分系统(APACHE-II)得分较低;然而,在肺炎发作时,与PaO₂/FiO₂>240的患者相比,他们的临床肺部感染评分(CPIS)、序贯器官衰竭评估(SOFA)得分、急性呼吸窘迫综合征标准及休克发生率更高,肺炎微生物学确诊率更低(分别为117例,69% 对71例,85%,p = 0.008)。在多因素逻辑回归分析中,PaO₂/FiO₂≤240与微生物学确诊率较低独立相关(校正比值比为0.37,95%置信区间为0.15 - 0.89,p = 0.027)。PaO₂/FiO₂与VAP微生物学确诊之间的关联较差,受试者工作特征(ROC)曲线下面积为0.645。两组之间初始治疗无反应情况及住院时间相似,而PaO₂/FiO₂≤240的患者医院死亡率更高。
在临床和影像学标准中增加PaO₂/FiO₂比值≤240无助于VAP的诊断。PaO₂/FiO₂比值>240不能排除这种感染。使用该阈值可能会低估VAP的发生率。