Department of Radiation Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL 33612, USA.
Case Western Reserve University, Department of Radiation Oncology, Cleveland, OH 44106, USA.
EBioMedicine. 2019 Sep;47:163-169. doi: 10.1016/j.ebiom.2019.08.019. Epub 2019 Aug 12.
Utilizing the linear quadratic model and the radiosensitivity index (RSI), we have derived an expression for the genomically adjusted radiation dose (GARD) to model radiation dose effect. We hypothesize GARD is associated with local recurrence and can be used to optimize individual triple negative breast cancer (TNBC) radiation dose.
TN patients from two independent datasets were assessed. The first cohort consisted of 58 patients treated at 5 European centers with breast conservation surgery followed by adjuvant radiotherapy (RT). The second dataset consisted of 55 patients treated with adjuvant radiation therapy.
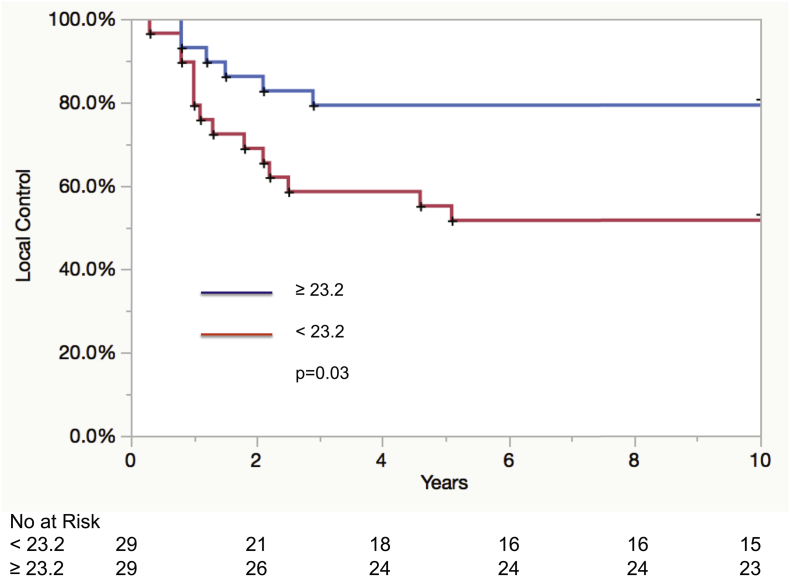
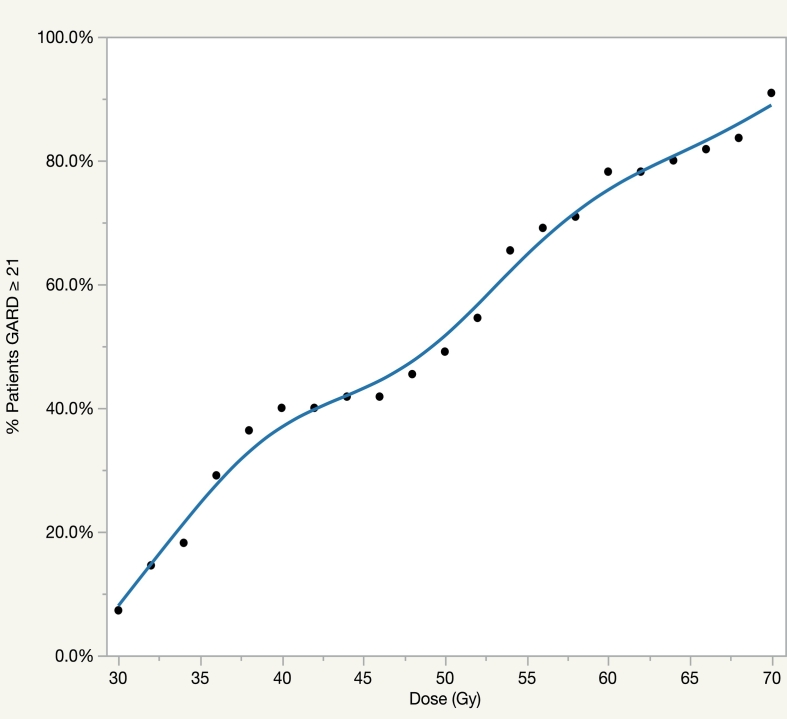
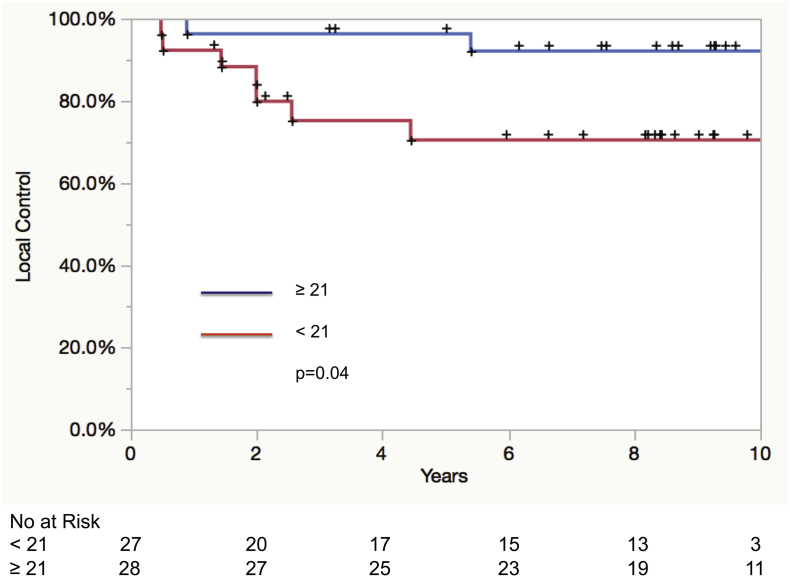
In cohort 1, multivariable analysis revealed that as a dichotomous variable (HR: 2.5 95% CI 1-7.1; p = .05), GARD was associated with local control. This was confirmed in the second independent dataset where GARD was the only significant factor associated with local control (HR: 4.4 95% CI 1.1-29.5; p = .04). We utilized GARD to calculate an individualized radiation dose for each TN patient in cohort 2 by determining the physical dose required to achieve the GARD target value (GARD ≥ 21). While 7% of patients were optimized with a dose of 30 Gy, 91% of patients would be optimized with 70 Gy.
GARD is associated with local control following whole breast or post-mastectomy radiotherapy (RT) in TN patients. By modeling RT dose effect with GARD, we demonstrate that no single dose is optimal for all patients and propose the first dose range to optimize RT at an individual patient level in TNBC.
利用线性二次模型和辐射敏感指数(RSI),我们推导出了一个用于模拟辐射剂量效应的基因组调整辐射剂量(GARD)表达式。我们假设 GARD 与局部复发相关,并可用于优化个体三阴性乳腺癌(TNBC)的放疗剂量。
评估了来自两个独立数据集的 TN 患者。第一组队列由 58 名在 5 个欧洲中心接受保乳手术后辅助放疗(RT)的患者组成。第二组数据集由 55 名接受辅助放疗的患者组成。
在队列 1 中,多变量分析显示,GARD 作为二分类变量(HR:2.5,95%CI:1-7.1;p=0.05)与局部控制相关。在第二个独立数据集得到了验证,其中 GARD 是唯一与局部控制相关的显著因素(HR:4.4,95%CI:1.1-29.5;p=0.04)。我们利用 GARD 计算了队列 2 中每个 TN 患者的个体化放疗剂量,方法是确定实现 GARD 目标值(GARD≥21)所需的物理剂量。虽然 7%的患者用 30Gy 剂量进行了优化,但 91%的患者将用 70Gy 进行优化。
GARD 与 TN 患者接受全乳或乳房切除术后放疗(RT)后的局部控制相关。通过用 GARD 对 RT 剂量效应进行建模,我们证明没有单一剂量适用于所有患者,并提出了第一个剂量范围,以优化 TNBC 个体患者的 RT。